A Resident in a Virtual Sea of Cardiology: My #AHA20 experience
As a current Internal Medicine resident and one of the youngest members of this year’s class of AHA Early Career Bloggers, my #AHA20 experience was equal parts thrilling, educational, and overwhelming. This was my first time attending the AHA Scientific Sessions and my second virtual conference experience after this year’s QCOR 2020 Scientific Sessions.
On a personal level, although it was convenient to virtually attend from my couch or work rather than fly across the country, I found it challenging to balance my time attending the conference with my clinical work: I was rotating on the Medical ICU at the time and was on call at times during the conference. Nevertheless, the more affordable and virtual nature of the conference and the ability to view sessions that I missed on-demand felt more inclusive to me. I also really appreciated the number of sessions dedicated to early-career trainees and attendings.
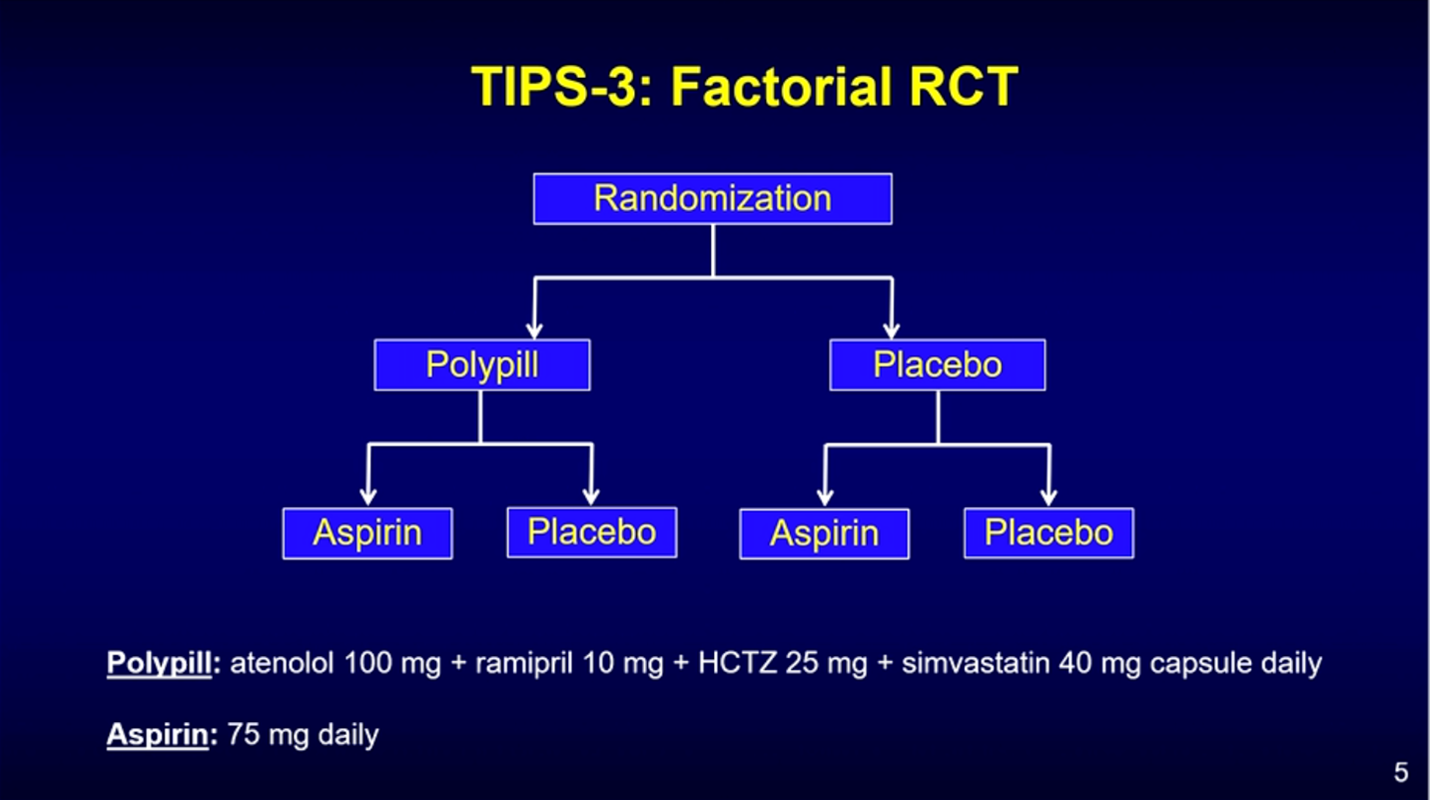
It was difficult at times to keep up with a large number of sessions or choose from the rich diversity of options, but overall I loved that there was a little something for everyone. I particularly enjoyed sessions about current state of care for heart failure, controversial trials such as OMEMI, STRENGTH and exciting, ingeniously-designed trials like SAMSON, and the big topic of #AHA20, the intersection of COVID-19 and cardiovascular health.
Most strikingly, the fact that the conference was all-virtual allowed for greater democratization of the dissemination of cardiovascular knowledge. In addition to all the wonderful content supplied by the AHA, there existed in parallel an equally comprehensive and all-consuming universe of discussion on Twitter. I found myself partaking in quite a few amazing Tweetorials or Twitter discussions about different topics presented at #AHA20! Any presentation you could think of was further broken down into bite-sized pieces of information by numerous expert cardiologists in the field. You could ask any question, and a leading expert in that area who had also viewed the presentation could answer your question to help you better understand the topic! As a trainee, I thought this made it easier for me to engage with other conference attendees in a medium with which I, as a millennial, am very comfortable. I also thought that the continued reinforcement of takeaways from the conference via my Twitter news feed helped me retain more knowledge than I usually do after I leave a conference. Although there was a deluge of content to wade through, the ability to re-watch sessions or re-read discussions about them made it easier to reinforce my learning.
Attending #AHA20 virtually as a trainee and getting to engage in the incredible online discussions both during and after sessions on Twitter was a very enriching experience for me. The ability to interact online and in real-time with other trainees, fellows, and attendings around the world made me feel as though the whole experience was more equitable, democratic, and accessible to early-career attendees like me. Finally, most of all, it engendered in me an even greater excitement to begin my Cardiology training in July 2021 and to continue conducting research that I can hopefully present at future AHA meetings.
“The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.”