Looking back at AHA21: reflection from a vascular neurology trainee
It has been just over a month since the American Heart Association Scientific Session 2021 concluded and I am elated to be a part of the Early Career Blogger program with a sponsored free access to the scientific sessions which also included the media pass!
My first thought after glancing at the schedule was, there is content for everybody to view and learn from, this includes researchers to nurses to clinical providers. Healthcare is vast and this session emphasizes that we do it as a community!
The virtual platform was very well organized which made it easy to navigate between the live sessions, posters, resuscitation science symposium and quality of care and outcomes sessions. I was truly fascinated by the quality of posters and presentations, with each one being unique. As an attendee, I had the option to pre-select the sessions of my choice, and add them to my calendar to keep track. The sessions covered topics from basic to clinical research and also included the most recent clinical trial updates. Apart from this, they discussed the role of social media on promoting cardiovascular health, emphasis on Diversion, Equality and Inclusion and Women’s Health. The sessions were very concise, with the most updated content and were moderated very well. The platform made it easy to ask questions without interrupting the presentation. Despite challenging times of a pandemic, there were many groundbreaking research, which tells us, science doesn’t stop and we are always learning and discovering to contribute to the betterment of quality of life and health.
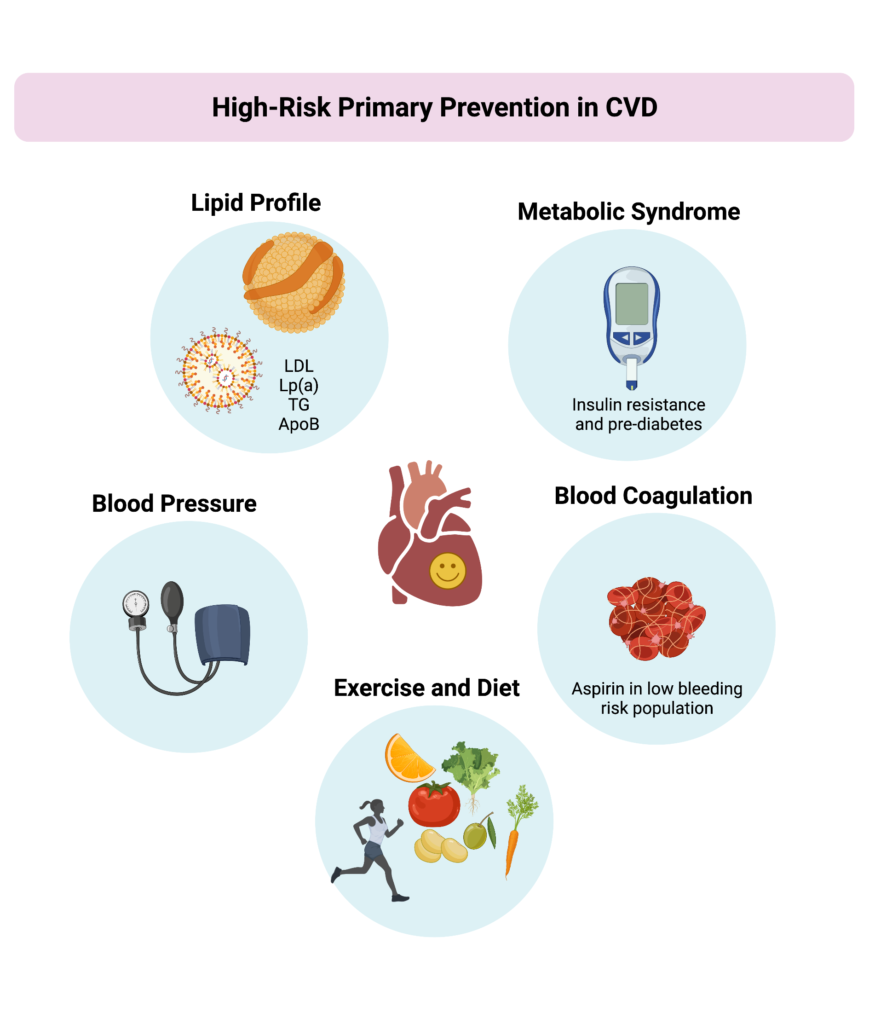
As we evolve, disease pathologies evolve, making them complex; There is always an overlap between systems, and we can never delineate one system from another and that’s when a platform like the American heart association brings the scientific community together and this year, to your computer screen, which helps researchers and clinicians learn and apply science to their practice.
As a vascular neurology trainee, I particularly enjoyed the sessions focusing on cerebrovascular health and the broad overlap between cardiovascular and cerebrovascular diseases. Some of the topics that drew my attention were, stroke epidemiology including the effect of hypertension on future brain health, gender-based outcomes after left atrial appendage occlusion, stress cardiomyopathy after aneurysmal subarachnoid hemorrhage, and case fatality associated with cardioembolic strokes, Atrial Fibrillation in 2021: Prepare for New Directions. Impact of COVID-19 on Cardiovascular Diseases, Secondary Stroke Prevention Guidelines: What Cardiologists Need to Know, Controversies in Stroke Management and Prevention and Updates in Stroke: Careers & Future Directions in Vascular Neurology (was privileged to blog on this session) to name a few. And it was not limited to listening to the lectures but felt even better when I apply it to patient care.
Apart from the scientific content, there were many educational discussions lead by seasoned panelists centered around, factors influencing various career vectors which addressed issues, events, and influential colleagues/mentors that contributed to their career choices with emphasis directed towards Early career attendees. The AHA journal editors gave us an insight on, What They Are Looking For? How to Publish? Opportunities for FIT’s to Be Involved and provided tips and advices for trainees to advance their career in publishing. One session that meant a lot to me was brought together by the ATVB Women’s Leadership Committee (WLC) who shared their own experiences on identifying and getting involved in volunteering activities such as, becoming a member of the early career committee, WLC program committee, leadership committee, as well as serving as a blogger etc. which were discussed in great detail.
It has only been a couple of months since being an AHA Fellow In Training and some of the perks that I’m already enjoying are, being able to engage with colleagues and mentors from around the world, volunteer opportunities with the AHA/ASA and gain national exposure, creating a pathway to Fellowship of the American Heart Association (FAHA), and making an impact in building healthier lives, free of cardiovascular disease and stroke.
The icing on the cake is the incredible opportunity to view all of the material with the on-demand access which is easy to access and can be viewed at your own pace. (https://ahasessions.heart.org/).
“The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.”