Bifurcations: EPISODE 3 – TAP TECHNIQUE
As the summer holidays wind down to the final few days, many of us are heading back to the routine of work, school and home. With the end of summer, my Bifurcation Series comes to a close as well. The final episode is the TAP technique.
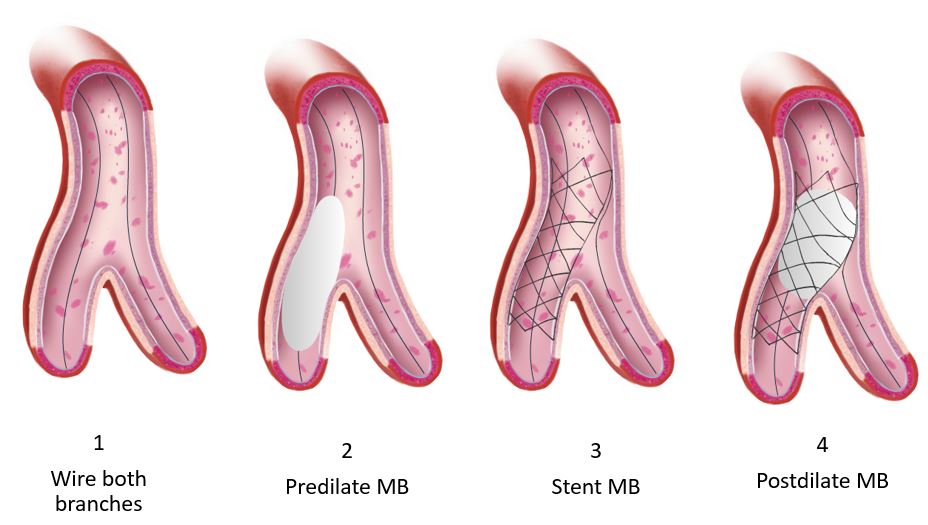
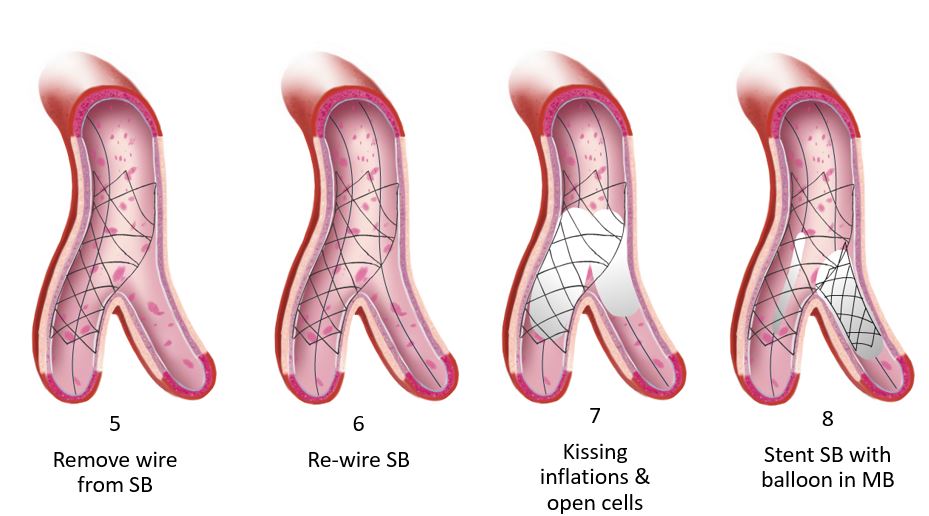
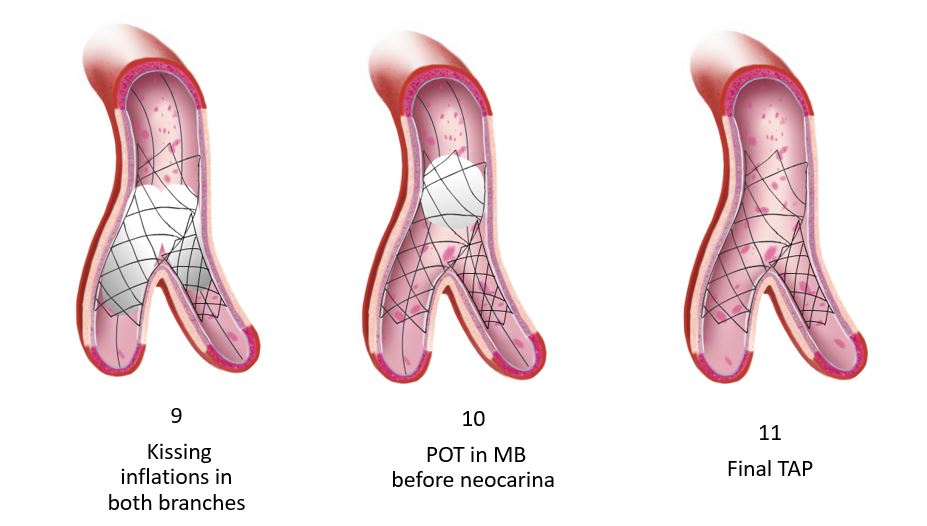
Operators find this to be the least cumbersome of all the 2-stent strategies. Many resort to it during emergencies as the access to the main branch (MB) is maintained throughout the procedure. The steps are fewer which ensures expeditious coverage of both vessels followed by the conventional optimization steps including kissing and proximal optimization with a non-compliant balloon. Similar to culotte, this strategy allows operators to start with a provisional strategy and convert to TAP should the need arise. In addition, there is minimal stent overlap. This technique is considered a modification of what was formally known as T-stenting. The primary limitation of the original T-stenting was missing the ostium of the side branch (SB). This geographic miss is what prompted many operators to perform minimal protrusion to mitigate in-stent restenosis at that missed segment. Hence the name TAP, T and small protrusion, was coined. Although this technique has been adopted worldwide, there are no large randomized trials with long term outcome data to reference. There are some published data; however, that are worth reviewing.
| Study | TAP strategy | Patients (n) | Unprotected left main stem |
Follow-up duration |
TVR | Definite stent thrombosis |
| Burzotta et al’ | Bail-out TAP in provisional | 73 | 37.0% | 9 months | 6.8% | 1.40% |
| Al Rashdan et al7 |
Systematic TAP | 156 | 10.3 % | 36 months (range 24-48 months) |
5.3% | 0.06% |
| Burzotta et a1 | Bail-out TAP in provisional procedures |
19 | 5.0% | 12 months | 5.3% | none |
| Naganuma et al | Bail-out TAP (type B dissection or TlMI <3 or stenosis >50% in the SB) |
95 | 18.9% | 36 months | 9.7% | none |
| ARTEMIS study10 |
Bail-out TAP (type B dissection or TlMI <3 or stenosis >75% in the SB) |
71 | 26.8% | 12 months | 8.5% | none |
| SB:side branch;TVR: target vessel revascularisation | ||||||
Burzotta et al, 2007
The modification of the T-stenting was first described in 2007 by Burzotta et al.1 It was evaluated in vitro and in two independent series of patients undergoing elective drug-eluting stent (DES) implantation on a bifurcation lesion. In vitro testing demonstrated perfect coverage of the bifurcation with minimal stent’s struts overlap at the proximal segment of SB ostium with a single layer stent struts. Sirolimus, paclitaxel, or zotarolimus DES were deployed in 73 patients (67% with Medina 1,1,1 lesions and 44% of unprotected distal left main disease) using the TAP technique. The procedural success was achieved in all cases. At 9 months the clinically-driven target vessel revascularization (TVR) was 6.8%. Since this was a pilot study, the investigators recommended larger outcome trials to further evaluate this technique. No comparison arm was available in this initial trial.
Al-Rashdan et al, 2009
In 2009 Al-Rashdan et al published their series of 156 consecutive patients who underwent TAP stenting.2 This was a single center study that resulted in a 99% procedural success rate and a major adverse cardiac events (MACE) free survival rate of 88% at 36 months average follow up. The TVR rate was 5.3%. Although to date this represents the largest cohort of TAP cases, the results are limited to a single center with no randomization which precludes further conclusions.
Burzotta et al, 2009
In 2009, Burzotta’s group prospectively enrolled 266 consecutive patients requiring treatment of a bifurcation lesion.3 The MB was treated with a DES and TAP was reserved as a bailout strategy. Only 19 of the total required a bailout 2-stent strategy. Nine percent of the total had unprotected left main disease. At one year, the MACE rate was 8.2%. A non-hierarchical analysis revealed a 0.4% cardiac death, 4.1% MI, 4.5% TVR and 2 of the total had probable stent thrombosis (ST). Given the small number of bailout 2-stent strategy arm, this study only demonstrates safety.
Naganuma et al, 2013
Naganuma et al retrospectively analyzed data of all patients who underwent TAP technique with DES between July 2005 and January 2012.4 A total of 95 patients were enrolled. Angiographic procedural success was achieved in all cases. A true bifurcation was found in 78.9% of those enrolled. The 3-year MACE, cardiac death or myocardial infarction, TVR and target lesion revascularization (TLR) rates were 12.9%, 3.1%, 9.7%, and 5.1%, respectively. No ST was observed in this cohort. Once again, the investigators recommend larger trials to make solid recommendations.
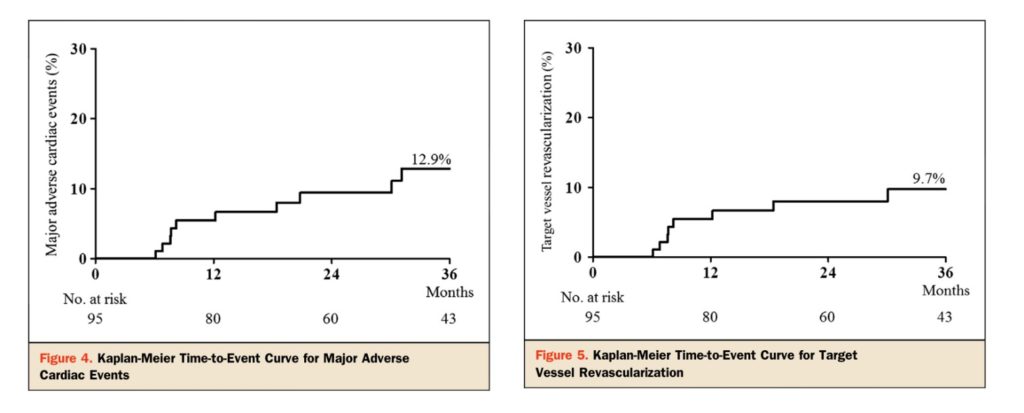
Naganuma et al, JACC Cardiovasc Interv. 2013;6:554-61.
ARTEMIS Study 2014
The ARTEMIS study was published in 2014.5 It evaluated the mid-term angiographic results of TAP as the bailout strategy in symptomatic patients who were treated with one-stent strategy (DES of the MB) and kissing balloon inflation of the SB who subsequently developed impingement of the branch. TAP was performed if residual diameter stenosis of SB was ≥75%, presence of ≥type B dissection or flow impairment of the SB occurred. A total of 71 patients were enrolled with a MEDINA classification 1,1,1 lesions occurring in 60% of the total. At 9 months, restenosis was occurred in 12.5% of the total. Late lumen loss in the MB and SB was 0.22 ± 0.19 and 0.34 ± 0.37 mm, respectively.
Dzavik et al, 2014
In 2014, there was much hype revolving around bioresorbable technology. Dzavik et al performed in vitro bifurcation stenting employing different modalities on synthetic arterial models.6 The everolimus-eluting bioresorbable vascular scaffold (Abbott Vascular, Santa Clara, California) (BVS) was used. A low-pressure final kissing balloon inflation was performed to complete the procedures. The results demonstrated that a single-stent technique optimally opened the SB without deforming the BVS in the MB. T or TAP-stenting covered the SB ostium completely. Culotte and crush with 2 BVS stents was successful; however, disruption was reported after the low pressure kissing inflation in one case. Investigators concluded that it was feasible to perform bifurcation stenting with BVS in large caliber vessels. They also recommended that a provisional strategy as the default. TAP or T-stenting with a metal DES is preferable. As the overall in vivo outcome data for BVS remains cautionary at best, the use of BVS outside clinical trials is not recommended whether for focal type A lesions or complex bifurcations.
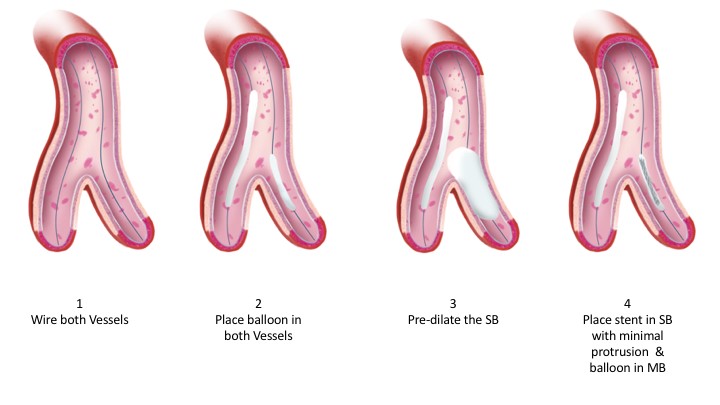
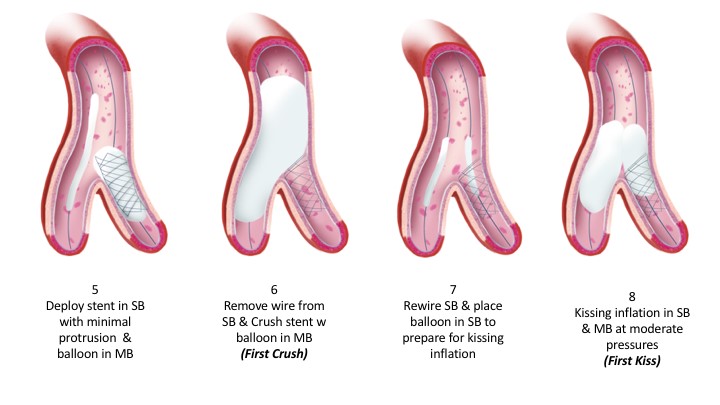
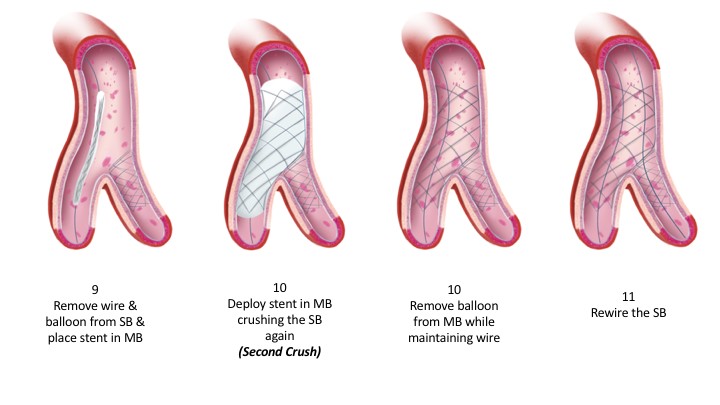
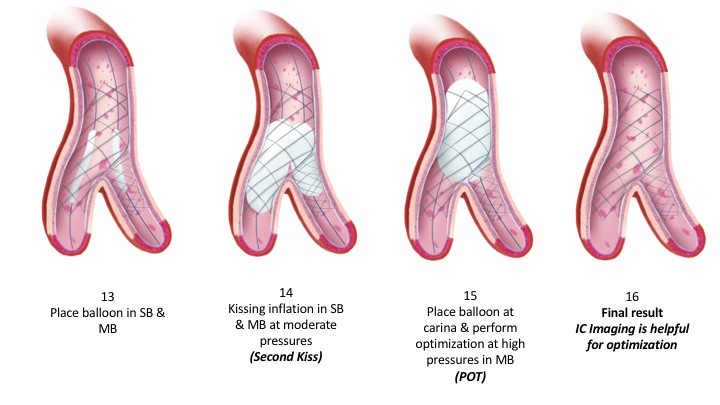
The technique itself is illustrated below. As mentioned earlier, it is one of the simpler 2-stent strategies. Like other strategies, appropriate sizing, positioning and optimization ultimately dictate the final angiographic and clinical outcomes. Intracoronary imaging facilitates these crucial steps. Yet, as with all interventions, judgment is the cornerstone of any successful procedure. When appropriate, and based on both Syntax score and clinical scores, surgical revascularization should be considered. When one opts for percutaneous revascularization, the indication for the procedure, its potential risks and complexity should be shared with the patient. For operators, judging the significance of the SB, the angle of the bifurcation, the size of both vessels and the need for mechanical circulatory support is valuable. Finally, complex bifurcation stenting is not for everyone. When appropriate, such complex procedures should be referred to expert operators for the best outcomes.
Animations/illustrations courtesy of Graphic Designer Dania Al-Shaibi
Email: [email protected]
References:
- Burzotta F, Gwon HC, Hahn JY, Romagnoli E, Choi JH, Trani C, Colombo A. Modified T-stenting with intentional protrusion of the side-branch stent within the main vessel stent to ensure ostial coverage and facilitate final kissing balloon: the T-stenting and small protrusion technique (TAP-stenting). Report of bench testing and first clinical Italian-Korean two-centre experience. Catheter Cardiovasc Interv.2007;70:75-82.
- Al Rashdan I, Amin H. Carina modification T stenting, a new bifurcation stenting technique: clinical and angiographic data from the first 156 consecutive patients. Catheter Cardiovasc Interv.2009;74:683-90.
- Burzotta F, Sgueglia GA, Trani C, Talarico GP, Coroleu SF, Giubilato S, Niccoli G, Giammarinaro M, Porto I, Leone AM, Mongiardo R, Mazzari MA, Schiavoni G, Crea F. Provisional TAP-stenting strategy to treat bifurcated lesions with drug-eluting stents: one-year clinical results of a prospective registry. J Invasive Cardiol.2009;21:532-7.
- Naganuma T, Latib A, Basavarajaiah S, Chieffo A, Figini F, Carlino M, Montorfano M, Godino C, Ferrarello S, Hasegawa T, Kawaguchi M, Nakamura S, Colombo A. The long-term clinical outcome of T-stenting and small protrusion technique for coronary bifurcation lesions. JACC Cardiovasc Interv. 2013;6:554-61.
- Jim MH, Wu EB, Fung RC, Ng AK, Yiu KH, Siu CW, Ho HH. Angiographic result of T-stenting with small protrusion using drug-eluting stents in the management of ischemic side branch: the ARTEMIS study. Heart Vessels.2014 Mar 14.
- Dzavik V, Colombo A. The absorb bioresorbable vascular scaffold in coronary bifurcations: insights from bench testing. JACC Cardiovasc Interv.2014;7:81-8.