Highlights from AHA20
AHA20 is wrapping up today with the final sessions. It’s been another excellent meeting with tons of new data that was presented. One consistent theme remains, debates continue to drive the conversation in the management of patients with cardiovascular diseases.
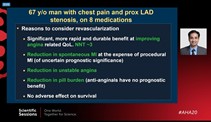
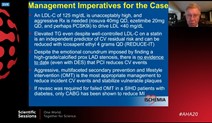
- The ISCHEMIA trial did not disappoint again. It led to great discussions regarding the contemporary management of patients with stable ischemic heart disease.”- First, the debate regarding PCI vs optimal medical therapy rages on. Dr. Sripal Bangalore and Dr. William Boden make their case for their approach to managing these patients.
The post ISCHEMIA world left us with burning questions about the optimal approach to imaging.
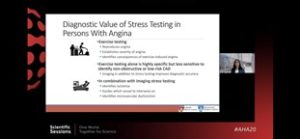
– CT vs SPECT for the evaluation of patients with SIHD
Guidelines will be surely updated after this landmark trial, but what remains certain is that a patient-centered approach to imaging is the key to optimal decision making.
- Optimizing GDMT in HF patients with more pills. How much is too much?
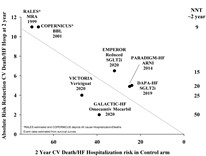
This year’s sessions added to our armamentarium in the management of patients with Heart failure and reduced ejection fraction (HFrEF). The GALACTIC-HF trial enrolled 8256 patients with LVEF <35% and pro-BNP >400 pg/ml to receive Omecamtiv Mercabil vs. placebo. With a primary composite outcome of cardiovascular death or CHF event, those enrolled to receive the selective cardiac myosin activator in addition to GDMT demonstrated a reduction in the primary composite outcome, driven by a reduction in CHF events.
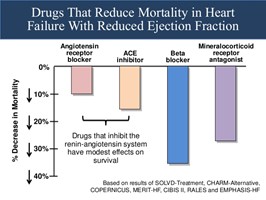
The results of this trial brought on questions regarding where newer agents in our HFrEF patients would rank in importance. Do we run the risk of polypharmacy and non-adherence with each newer agent? How much bang for our buck can we expect to receive?
Key takeaways from the discussions regarding GDMT include:
- Early initiation and up-titration of medical therapy improve outcomes in HF patients.
- Recognize signs of worsening HF and decompensation
- Referral to advanced heart failure cardiologists when you need help.

Debates trigger conversations, conservations lead to action. Action in this setting leads to improved patient outcomes. AHA 2020 Scientific Sessions was no different and provided great examples of this rhetoric.
One thing not up for debate at this year’s Scientific Sessions was clear. It was the call to action against structural and institutionalized racism, the fight for diversity, equity, and inclusion for all. From the opening address to the final sessions, AHA 2020 made it a point to bring these conversations to the forefront to impact change. At the end of these 5 days, I feel re-invigorated and optimistic that our actions moving will speak louder than our words. Here’s to hoping we can meet again in person at next year’s Scientific Sessions.
“The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.”