A sigmoid-shaped interventricular septum (SIS) is generally considered a normal part of the aging process and is of little clinical significance. However, certain patients with SIS may experience clinical symptoms, such as dyspnea upon effort and different types of cardiac arrhythmias. SIS is frequently observed on transthoracic echocardiography (TTE) and in cardiac magnetic resonance (MR) imaging modality in daily clinical practice. However, nothing usually occurs in subjects with SIS, and the clinical significance of the presence of SIS is unclear.
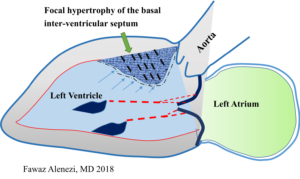
The precise mechanisms leading to isolated SIS have yet to be determined, but plausible reasons exist as to why the basal septum might be uniquely susceptible to hypertrophy. For example, Laplace’s law states that the larger a vessel’s radius, the larger the wall tension required to withstand internal fluid pressures. Because the longitudinal fibers of the basal septum have some of the largest radii in the human heart, they would be expected to experience the greatest inward component of wall stress. This is compounded by the fact that the basal septum is the last part of the ventricle to be electrically activated, so contractions from other myocardial segments further increase its wall stress (Fig. 1). Moreover, the additional load created by pressure from the right ventricle exerts additional stress on the septum. Therefore, it is conceivable that the basal septum hypertrophies earlier than other LV regions in response to increased afterload as it already operates under higher loading conditions.
Prospective studies suggest that up to 20% of cardiovascular cohorts may have isolated SIS. Some researchers have reported that the cause of SIS may be aging or arteriosclerosis. This may involve a change in the spatial relationship between ascending aorta (AA) and left ventricle (LV) due to elongation or tortuosity of arteriosclerotic AA. An alternative hypothesis suggests that SIS may be a form of cardiomyopathy. However, there is no evidence to support such a hypothesis due to the limited capabilities of traditional TTE. Use of other diagnostic approaches like CMR may be needed where characteristics of LV myocardium and the spatial relationship between AA and LV and degree of arteriosclerosis of AA can be evaluated simultaneously.
It is known that LV hypertrophy with different remodeling patterns is one of the major cardiac manifestations of hypertensive heart disease, and echocardiographic LV hypertrophy could be detected in 20-40% of patients with arterial hypertension. However, there are often no specific echocardiographic features for hypertensive patients at the early stage of disease. Previous echocardiographic studies have described asymmetric septal hypertrophy with a localized septal thickening at the basal-mid portion in patients with hypertrophic cardiomyopathy or aortic valve stenosis.
Basal-septal hypertrophy may also occur in a subset of older normal subjects, with normal wall thickness (WT) elsewhere, and is considered to be an age-related anatomic variant. This morphologic echocardiographic sign is termed as septal bulge (SB), sigmoid septum, or discrete upper septal thickening or knuckle. A large community-based population study reported that SB was documented frequently in elderly individuals with higher systolic blood pressure (BP). It was shown that the overall prevalence of SB was 1.5% and was markedly higher (18%) in the eighth decades of life.
Although pathologic and echocardiographic observations have indicated that SB is a structural response in hypertensive patients, the nature and significance of the SB in subclinical arterial hypertension was never investigated. In addition, despite the fact that BP can be easily measured, AH sometimes cannot be diagnosed due to the underreported BP reading in the casual or self-measured BP measurement. BP measurement with appropriate tools is essential to diagnosing AH early as well as to guiding AH management. It has been shown that, besides resting BP measurement in the office, arterial hypertension could be clinically diagnosed by 24-hour ambulatory BP monitoring (ABPM) as well as exercise stress test in some resting normotensive individuals.
Focal hypertrophy of the basal inter-ventricular septum can be seen in up to 20% of cardiac patients without HCM, being more prevalent in the elderly and hypertensives. While it’s anatomical location plausibly renders it more susceptible to hypertrophy, evidence suggests that the basal septum enlarges mainly due to pressure overload from hypertension. This discrete upper septal hypertrophy is associated with exertional LVOT obstruction and SOB, and appears symptomatically amenable to β -blockade. While diastolic dysfunction likely also contributes to symptoms in this condition, the data to date are equivocal. Focused analyses conducted using a consensus definition of SB, in patients undergoing simultaneous assessment of myocardial systolic and diastolic performance during physiological exercise, are needed to further understand the clinical relevance of this entity.

Dr. Fawaz Abdulaziz M Alenezi is a Clinical Imaging Fellow at the Duke University Health Systems. He conducts medical research on the derivation and validation of novel echocardiographic approaches to myocardial deformation and a new echocardiographic technique which assists patients with heart ventricular function.