
Drs. Yusuf and Pais from the Population Health Research Institute in Ontario, Canada presented data from the International Polycap Study (TIPS)-3 study[1] as part of the Late-Breaking Science Session: Bending the Curve for CV Disease-Precision or PolyPill? at the AHA20 Scientific Sessions. The aim of this study was to try to simplify primary prevention via a ‘polypill’ (Polycap) for not only cardiovascular disease (CVD) but also conditions with similar risk profiles, such as breast cancer and osteoporosis. The polypill contains 3 blood pressure medications (hydrochlorothiazide (25mg), atenolol (100 mg), ramipril (10mg)) and a statin (simvastatin (40 mg). They are searching for a ‘magic bullet’ if you will, to reduce these chronic diseases with a high burden in the U.S and around the world. Precision medicine can be effective but is costly. The use of a polypill can help to reduce the curve of disease burden or at least shift it towards reducing the number of high cardiovascular risk people worldwide.
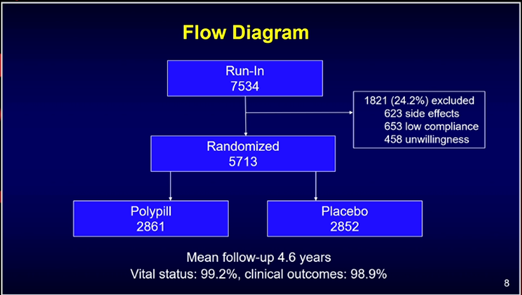
This study enrolled 5,713 middle aged participants from 10 different countries (Including India, Tanzania, and Tunisia). With a 2x2x2 factorial design, randomized controlled trial investigators aimed to assess the effectiveness of PolyCap the ‘Polypill’. Participants were eligible for the study if they did not have prior heart disease or stroke. Participants were excluded if they had any contraindications to the study medications, low and symptomatic hypotension, history of malignancy, and inability to attend follow-up. There were three treatment arms. The participants were randomized to the polypill vs placebo. In addition, participants were also randomized to receive aspirin (75 mg) and vitamin D (60,000 IU monthly) each vs. placebo. The primary outcome was major cardiovascular disease (CVD) (CV death, non-fatal stroke, non-fatal MI), plus heart failure, resuscitated and cardiac arrest, or revascularization with evidence of ischemia in participants taking Polycap versus placebo. For the aspirin arm, the primary outcome was composite CV events ( CV death, MI or stroke) and cancer. For vitamin D arm, the primary outcome was risk of fractures in participants taking Vitamin D. The data presented at AHA2020 Scientific Sessions was for the Polypill with and without aspirin alone vs. placebo. This was an intention to treat analysis. Investigators also conducted a sensitivity analysis for those who were not able to adhere to medications and identified outcomes at 30 days in the active and placebo groups.
After a follow-up time up to 5 years, the investigators enrolled a cohort of 53% women with intermediate CVD risk based on the IH (INTERHEART) risk score (1.5 % per year risk of CVD). For participants taking the Polypill vs. placebo, there was a significant mean reduction in systolic blood pressure by approximately 5 mm Hg and LDL-C by approximately 19 mg/dL. There was a 21% reduction in the primary outcome; however, overall mortality was not significantly different. The greatest reduction was seen with revascularization with a 60% reduction compared to the placebo. There was a reduction in cancer outcomes as well, but not significantly; this is likely related to low events. The bleeding risk profile was low. With the combination of aspirin and the Polypill, there was a 31 % risk reduction compared to placebo, aspirin alone, and the Polypill alone ( compared to 14% with aspirin vs. placebo alone) in the composite primary outcome but no overall mortality benefit. This was mainly driven by a reduction in stroke. CVD death and cancer were significantly reduced by 30% compared to placebo. There was also a reduction with systolic blood pressure and LDL-C as seen with the Polypill alone. Aspirin alone did not show any difference with major/minor bleeding or GI bleeding likely related to having a run-in period and a lower dose of asa (75 mg). In both cases, the heart failure rate was higher in both groups but this was not significant with a wide confidence interval with low event. It is important to note that lifestyle modification teaching was also instituted and the reduction in outcomes is therefore contributed to both the medication and education. One main issue was adherence to the medications (just two pills) up to 43%! This was in part due to COVID19 by the end of the study. Per the sensitivity analysis, the outcomes of those with some adherence (<30 days) were still significantly lower than the placebo. Taking something for even a short period of time is better than nothing.
The authors highlight the significant limitation of non-adherence which can create a selection bias in the data. However, if only half eligible people adhere to this regimen, 3-5 million CVD events can be avoided each year globally. They note that the challenge of adherence lies in social determinants of health, which have a great impact on CVD outcomes. More needs to be done to understand cost-effective ways to ‘bend the CVD curve’ by identifying effective implementation programs (including telehealth) to distribute this combination of medications.
References:
Joseph et al. The International Polycap Study-3 (TIPS-3): Design, baseline characteristics and challenges in conduct. Am Heart J. 2018 206:72-79