“Wisdom consists of the anticipation of consequences”
Norman Cousins
I recently saw Mr. John Doe for atrial fibrillation (AF). Well into his eighties, he enjoys a good quality of life. This elderly gentleman is mostly unaware of his paroxysms of AF. However, he had also suffered a stroke in the past, and as such was managed with warfarin. He was lucky. Recently, he experienced a gastrointestinal hemorrhage, requiring temporary reversal of his anticoagulant in addition to receiving a few pints of blood. There were no apparent clinical triggers for this event. Mr. Doe is not a fictional person but is a typical example of what is a common clinical dilemma: how best to protect against stroke in a patient who is at high risk, yet becomes intolerant to warfarin.
Previously, these patients were commonly switched to aspirin alone as a poor alternative to anticoagulation. Most clinicians would feel apprehensive of taking a gamble switching to novel oral anticoagulants which do not have available reversal agents (at the time this blog was written).
So, what then?
Enter the “Watchman.”
The majority of thromboembolic strokes in patients with AF originate in the left atrial appendage (LAA). The function of this structure is to assist with atrial transport, however during AF, atrial blood flow becomes impaired and stasis can occur in the LAA leading to thrombus formation at this location. Fragmentation and embolization of thrombi can lead to stroke, which is commonly disabling. The presence of comorbid factors such as diabetes, heart failure among other clinical variables can further increase this risk [1].
The last several years has witnessed the development and refinement of procedures referred to as left atrial appendage occlusion. Although there are several of the devices available worldwide, I will refer to the WATCHMAN system which is approved for use in the United States. In brief, the WATCHMAN device resembles a small umbrella (Figure 1). The FDA approved the device for the purpose of preventing embolic stroke with non-valvular AF. The available data that lead to its approval implies a non-inferiority to warfarin [2,3]

Figure 1. (accessed from www.bostonscientific.com; www.modernhealthcare.com)
The method of device introduction is via a femorally placed venous sheath delivered transseptally (from right to left atrium). The destination of the device is the ostium of the LAA (Figure 2). The ultimate goal of the procedure is to totally exclude the LAA from the chamber, thus preventing flow into and from the LAA, in effect precluding thrombus formation. The procedure is performed with the guidance of transesophageal echocardiography, and typically under general anesthesia. The duration of the implant typically does not exceed an hour. Patients are continued on warfarin during the initial perioperative phase.
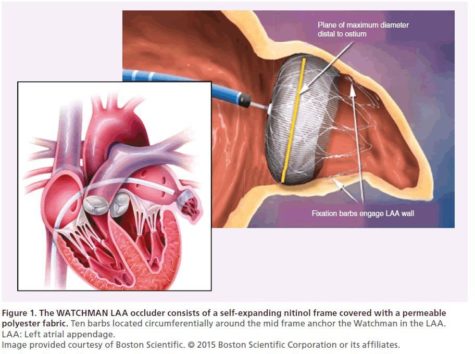
Figure 2. (Accessed from www.bostonscientific.com; openaccessjournals.com)
Generally, after a forty-five-day period, transesophageal echocardiography is repeated to confirm the absence of peri-device leaks and verify device endothelialization. If the results are favorable, patients can often stop warfarin and switch to antiplatelet therapy. Presently, the available evidence compares WATCHMAN to warfarin, and comparisons to other anticoagulants is lacking.
It appears that enthusiasm for the WATCHMAN appears to be growing. For patients who require long-term warfarin use, but are at risk for hemorrhagic complications, this device appears to be a very good option. Cumulative experience will invariably lead to further improvements in design and greater safety [4,5].
References
- Lip GY, Lane DA. Stroke prevention in atrial fibrillation: a systematic review. JAMA. 2015;313:1950-62
- Holmes DR Jr, Kar S, Price MJ, Whisenant B, Sievert H, Doshi SK, Huber K, Reddy VY Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial.J Am Coll Cardiol. 2014;64:1-12
- https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=2 81&bc=ACAAAAAAAgAAAA%3d%3d&
- Reddy VY1, Doshi SK2, Kar S3, Gibson DN4, Price MJ4, Huber K5, Horton RP6, Buchbinder M7, Neuzil P8, Gordon NT9, Holmes DR Jr10; PREVAIL and PROTECT AF Investigators. 5-Year Outcomes After Left Atrial Appendage Closure: From the PREVAIL and PROTECT AF Trials.J Am Coll Cardiol. 2017;70:2964-2975
- Obeyesekere MN.Watchman Device: Left Atrial Appendage Closure For Stroke Prophylaxis In Atrial Fibrillation.J Atr Fibrillation. 2014; 7: 1099
Christian Perzanowski is an electrophysiologist in Tampa, FL. His main interests are in ablation techniques for atrial fibrillation and device therapy for congestive heart failure. He reports no conflicts of interests.

Apollo Beach, FL (05/17, CP)