Does a polypill obviate the need for behavioral changes? Absolutely not. As a physician training in Cardiology, I spend a sizeable part of my time discussing achievable weekly nutritional goals with patients in addition to stressing the importance of medication adherence. I ask myself after watching the “Bending the Curve for CV Disease- Precision or Polypill,” would I recommend a pill that can treat both hypertension and hypercholesterolemia and decrease the risk for CV disease? Certainly, this would make medication adherence for our patients much simpler, especially with the combination of atenolol, ramipril, hydrochlorothiazide, and simvastatin into one pill.
The International Polycap Study (TIPS-3) presented by Drs. Prem Peis and Salim Yusuf was a double-blinded, randomized trial of more than 5,700 adult men and women at increased CV risk with an intervention of the once-daily polypill, aspirin, combination of both or placebo (see figure). Endpoints of CVD events included CV death, non-fatal stroke, non-fatal MI, heart failure, resuscitated cardiac arrest, or arterial revascularization.
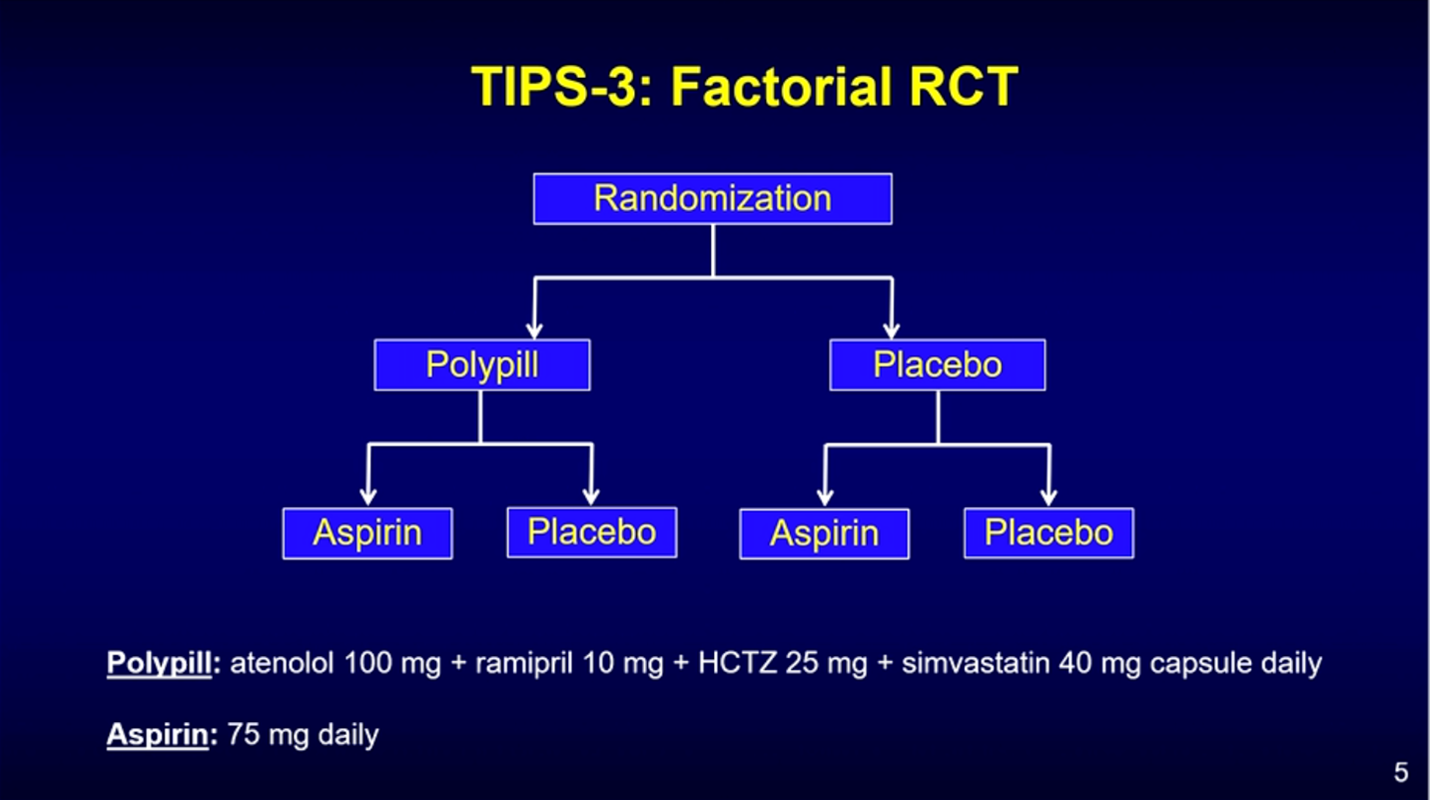
To summarize the results, 5-year outcomes found that the polypill was superior to placebo in decreasing systolic blood pressure, LDL-C, and non-fatal CV events in mostly Southeast Asian participants. Low-dose aspirin resulted in lower stroke risk and the additive effect of aspirin to the polypill had a higher reduction in nonfatal CV events when compared to the double placebo arm. The side effects of the intervention group included dizziness and hypotension.
As I return back to clinical responsibilities, I reflect on the AHA Scientific Sessions with particular attention to this polypill. Would you recommend a pill that was cost-effective that decreased pill-burden in your patient? I think I would but not at the cost of leaving behind crucial behavior changes that are integral for health and well-being.
More importantly, the following slide resonated with me the most and I believe conceptualizes a comprehensive framework for prevention and precision medicine:
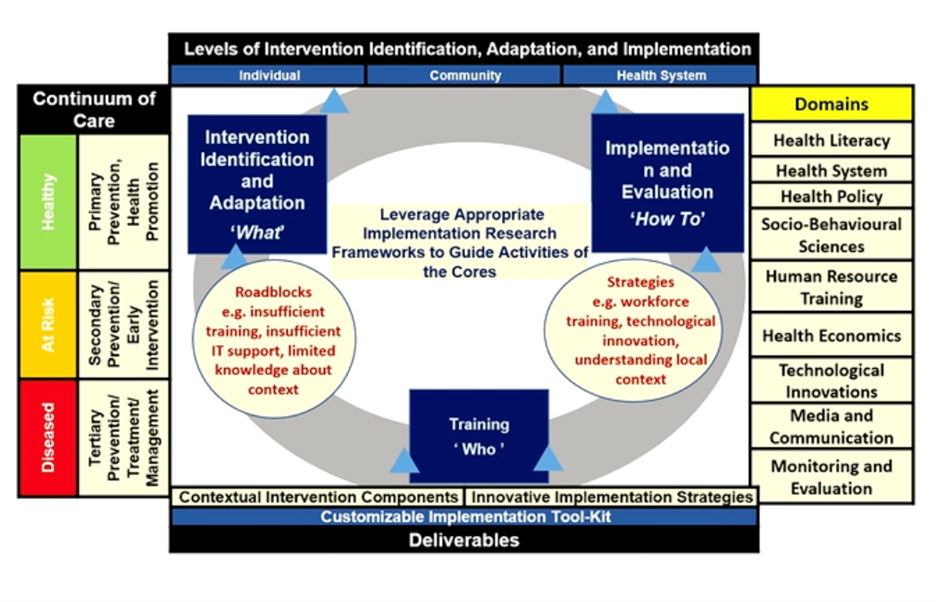
The takeaways here are that there is a continuum of care across a spectrum of healthy, at risk, and diseased patients we see on a daily basis. Each group in this spectrum requires an individualized, community, and health system approach to intervention and implementation of decreasing cardiovascular risk. The domains needing to be addressed are part of a long list but each important in their own right:
Health Literacy
Health System
Health Policy
Socio-Behavioral Sciences
Human Resource Training
Health Economics
Technological Innovations
Media and Communication
Monitoring and Evaluation
With this framework in mind, I challenge myself and you all to think more deeply about how we might integrate universal standards along with individually-tailored preventative interventions when managing our patients. Our day-to-day clinic experience can at times lull us into the feeling of an unchanging routine, however this presentation was a great reminder of future opportunities to probe further to apply novel universal approaches while also seeking to understand individual patients’ health behavior needs and pushing individualized medicine further in the domain of CV prevention. This will be accomplished through quality care projects, educational work, health equity advocacy, and investigative research.
Take care and be well.
References:
https://www.nejm.org/doi/full/10.1056/NEJMoa2028220
“The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.”