Better understanding how depression, social isolation, and other psychosocial determinates of health interact with cardiovascular disease is a rapidly growing field of research. Unpacking the relationship between brain function, cardiovascular physiology, and health outcomes is no simple feat. A number of new studies presented on Saturday, November 16th at the “Depression and Psychosocial Influences on Cardiovascular Disease” poster session during this year’s American Heart Association Scientific Sessions shed new light on this topic.
Crystal Cene and her team at the University of North Carolina presented findings from the Womens Health Initiative Study (WHI) showing a correlation between social isolation and heart failure. In their analysis, they found that socially isolated woman had a 19% higher risk (HR of 1.19; CI 1.03 – 1.39) of developing heart failure over a median follow-up of 15 years1. These findings complement work published earlier this year by Anne Vingaard Christensen and colleagues at Copenhagen University Hospital2. Among 13,442 patients with ischemic heart disease, arrhythmia, valvular disease, or heart failure, loneliness predicated all-cause mortality in men (HR 2.14; CI 1.43 – 3.22) and women (HR2.92, CI 1.55 – 5.49). Given that we now have evidence that loneliness or social isolation puts patients at risk for heart failure and puts patients with heart failure at risk of all-cause mortality, there is all the more need to better understand this relationship.
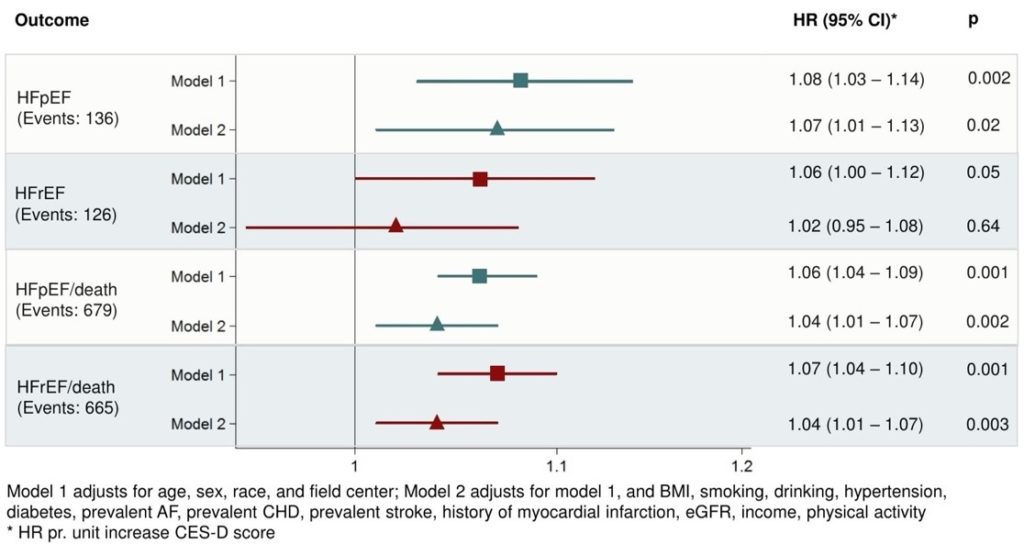
 Two other groups of researchers presented similar findings with depression and heart failure. An analysis of The Atherosclerosis Risk in Communities Study (ARIC) presented by Katja Vu from Brigham and Women’s Hospital found a relationship between depression and incidence of heart failure with preserved ejection fraction (HR 1.07; CI 1.02 – 1.13) among older adults (mean age 75 years) of both sexes3. However, there was no such relationship with incidence of heart failure with reduced ejection fraction [Figure 1]. Yosef Khan from the American Heart Association presented National Health and Nutritional Examination Survey (NHANES) data suggesting that depression increases risk of heart failure, coronary disease, or cerebrovascular disease even after adjusting for Life’s Simple 7: physical exercise, heart healthy diet, weight, blood pressure, cholesterol, blood sugar, and tobacco use4.
Two other groups of researchers presented similar findings with depression and heart failure. An analysis of The Atherosclerosis Risk in Communities Study (ARIC) presented by Katja Vu from Brigham and Women’s Hospital found a relationship between depression and incidence of heart failure with preserved ejection fraction (HR 1.07; CI 1.02 – 1.13) among older adults (mean age 75 years) of both sexes3. However, there was no such relationship with incidence of heart failure with reduced ejection fraction [Figure 1]. Yosef Khan from the American Heart Association presented National Health and Nutritional Examination Survey (NHANES) data suggesting that depression increases risk of heart failure, coronary disease, or cerebrovascular disease even after adjusting for Life’s Simple 7: physical exercise, heart healthy diet, weight, blood pressure, cholesterol, blood sugar, and tobacco use4.
Call to action:
These provocative findings leave us with many questions: What mechanisms are responsible for poor outcomes among patients with social isolation or depression? Does access to care or medication adherence mediate these effects? Would interventions to reduce social isolation or depression improve cardiovascular outcomes in the long-run? There is a lot left to discover in this bio-psychosocial model, but I for one am looking forward to future work in the field.
References:
- CW Cene et. al. Social Isolation Independently Predicts Incident Heart Failure Among Older Women: Findings From the Womens Health Initiative Study. Poster Presentation, American Heart Association 2019 Scientific Sessions, Philadelphia, PA, November 16-18, 2019 (https://www.abstractsonline.com/pp8/#!/7891/presentation/29740)
- Christensen AV, et al. Heart 2019;0:1–7. doi:10.1136/heartjnl-2019-315460
- K Vu et. al. Depressive Symptoms, Cardiac Function, and Risk of Heart Failure With Preserved or Reduced Ejection Fraction in Late Life: The Atherosclerosis Risk in Communities (ARIC) Study. Poster Presentation, American Heart Association 2019 Scientific Sessions, Philadelphia, PA, November 16-18, 2019 (https://www.abstractsonline.com/pp8/#!/7891/presentation/29738)
- Y Khan et. al. Depression and Non Fatal Cardiovascular Diseases Among Adults in the United States. Poster Presentation, American Heart Association 2019 Scientific Sessions, Philadelphia, PA, November 16-18, 2019 (https://www.abstractsonline.com/pp8/#!/7891/presentation/29739)
The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.