Although the awareness and treatment of hypertension has increased steadily over the past decade, it is estimated that approximately 50% of patients are still not adequately controlled. However, blood pressure measurement techniques vary widely and results from studies are difficult to compare. Further, office BP measurements depend on time, resources, and equipment.
In our referral Cardiology-Hypertension Clinic blood pressure is measured in different ways by different providers:
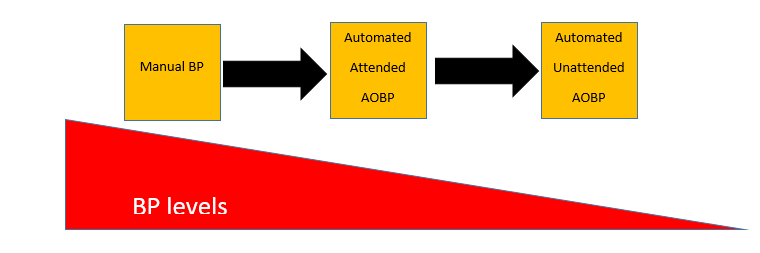
- Manual
- attended automated office BP (AOBP) with 3 consecutive readings (Omron) or
- unattended attended automated office BP (AOBP) with 3 consecutive readings (Omron) or 6 consecutive readings (BPTrue).
“Attended” means that trained personnel stays in the room, while in unattended measurements trained personnel leaves the room and monitors are either programmed to take 3 or 6 consecutive readings.
These different approaches make it difficult to compare BP levels and to adjust medication to achieve target BP.
So what is the best way to measure blood pressure and which is the one we should stick to?
It is known that BPs taken manually can differ from those taken using an automated device in the clinic or office. Several studies have shown that manually taken BPs can be higher than AOBP. Further, many clinicians prefer AOBP over manual BPs since it is an easy way to check BP several times.
With advances in technology, unattended AOPB measurements are possible. Research suggests that unattended blood pressure measurements are significantly lower than attended blood pressure measurements.
Clinical trials using AOBP usually pre-specify how to measure BP i.e. either attended while trained personnel stays in the room or unattended i.e. medical staff comes back after a few minutes and retrieves BP readings.
The importance of a consistent way to measure BP has come under scrutiny in the SPRINT study.
Although blood pressure measurements in this study were obtained using an automated measurement device, there were substantial differences in the methods used by the different SPRINT centers. In particular, medical staff were inconsistently present or absent when blood pressure readings were taken, between centers and perhaps within centers.
Blood pressure in SPRINT was defined as the average of three measurements taken with an automated measurement device. But until now it has not been entirely clear whether these measurements were obtained in the presence or absence of medical staff.
Results of a survey for the SPRINT trial showed that patients were completely alone during the measurement period at 43% of the sites and were alone (unattended) for part of the time at 29% of the sites. However, within sites significant internal variation in their BP measurement techniques (unattended and attended AOBP) may have occurred.
What is clear is that there are a variety of methods currently employed to measure BP in clinical trials and in the office, and that technique, environment, and equipment can influence BP levels obtained.
To put that in perspective for clinical practice we should take this into consideration and report how BP was measured when we communicate with our patients or colleagues.

Tanja Dudenbostel is an Internist, Hypertension Specialist within Cardiology at the University of Alabama at Birmingham where I divide my time as an Assistant Professor between clinical research and seeing patients in cardiology.