Right Ventricular Structure and Function
The effect of anticancer medication on the (LV) function and structure has been extensively investigated in comparison to the right ventricle (RV). In general, it’s known that deterioration of RV function is associated with significant morbidity and mortality. However, despite advancement in echocardiographic and other imaging techniques, the RV assessment remains challenging in comparison to the LV. In this short statement I will summarize some of the RV characteristics and distinguish
First: The right and left ventricles have distinct morphological difference. Embryologically, the RV is derived from the secondary heart field whereas the LV is derived from the primary heart field. The RV has crescentic non-ellipsoidal configuration and three anatomic divisions (an inlet region, trabeculae free wall/ apical region and an outflow tract). In addition, the RV mass and wall thickness is about 1/3 of the LV.1
Second: The RV has different cardiodynamics:
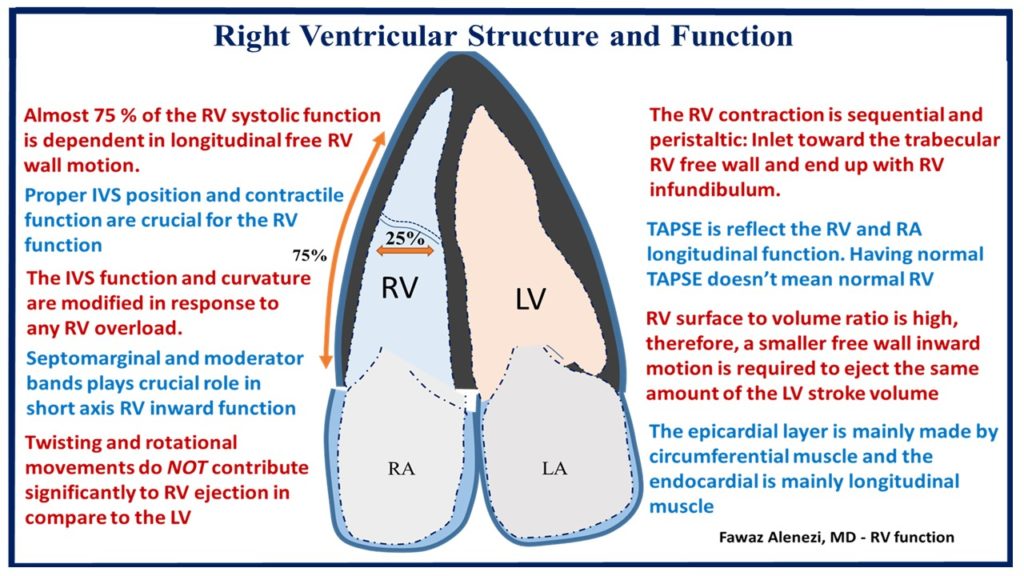
- The RV contraction is sequential and peristaltic: started by the RV inlet toward the trabecular free wall and end up with infundibulum. Rather than the LV contraction which is uniform, longitudinal and torsion. In case of RV volume or pressure overloads it’s become more uniform in contraction.
- The RV has 3 separate mechanisms of contraction:1
- Free wall inward movement “bellows – like effect) that is dependent on the moderator/ septomarginal band’s position and contractility.
- Contraction of longitudinal fibers (shortens long axis TV annulus toward apex)
- Traction of free wall from septal LV attachments.
- Shortening of RV is much greater longitudinally (75%) than radially (25%). The radius of the curvature and RV surface area do not change appreciably.
- The epicardial layer is mainly made with circumferential muscle and the endocardial is mainly made with longitudinal muscle loop. In comparison, the LV has helix that formed by ascending and descending obliquely oriented loops. Thus, twisting and rotational movements do NOT contribute significantly to RV ejection in compare to the LV.
Third: The RV surface/ volume ratio is high, therefore, a smaller free wall inward motion is required to eject the same amount of the LV stroke volume. Also, the RV isovolumetric contraction and relaxation are shooter than the LV, simply, because the pulmonary artery diastolic and RV filling pressure are low. In addition, about 30% of the RV systolic and stroke volume occur due to the interventricular septum (IVS) by the phenomena called “systolic ventricular interdependence.”1
Forth: Proper IVS position and contractile function are crucial for the RV function. The IVS function and curvature are modified in response to any pressure or volume overload. Under normal RV pressure, the IVS is concave toward the LV in both systole and diastole. However, in patient with pulmonary hypertension the IVS curvature become more convex shape which may help the RV to eject more blood against high pulmonary pressure.1,2
Fifth: RV failure occurs under almost two conditions, excessive RV afterload and IVS dysfunction. The most important determinant of the RV function is:1,2
- RV afterload (Vascular resistance and compliance)
- RV contractility (systolic function)
- The coupling of RV contractility to RV afterload
- Pericardial constraint/RV-LV diastole interactions
The RV function and structure assessment is challenging. An ideal index of contractility should be independent of afterload and preload, sensitive to change in inotropy, independent of heart size and mass, easy and safe to apply, and proven to be useful in the clinical setting.1,2 Invasively, the gold standard measure of RV function still the volume/ pressure relationship. The most clinically used measures of RV systolic function (RVEF, RV FAC, TAPSE, S’ tricuspid valve velocity, RV SV, strain and RVMPI) are load dependent. Just like the LV, we are slowly evolving into global longitudinal strain (GLS). Important to remember that LV GLS is a surrogate of LV ejection fraction (LVEF) and the dichotomy between the LVEF and GLS can be explained by global circumferential strain (GCS), (Figure 1).
Figure 1: Right ventricular structure and function
References:
- François Haddad, MD; Sharon A. Hunt, MD; David N. Rosenthal, MD; Daniel J. Murphy, MD Right Ventricular Function in Cardiovascular, Part I. Circulation 2008, 117:1436-1448
- François Haddad, Ramona Doyle, Daniel J. Murphy and Sharon A. Hunt. Right Ventricular Function in Cardiovascular Disease, Part II. Circulation 2008, 117:1717-1731