AHA 2020 Delivers on Virtual Conference Experience
As we near the close of the American Heart Association’s 2020 Scientific Sessions, I’d like to reflect on the virtual conference experience. I must admit, despite the high quality research and programming schedule, I was skeptical going into this year’s virtual conference. It was my first (of many?), and I had reservations about the ability of any organization to recreate the live experience that we all love so dearly. Looking back, the AHA put on a phenomenal show, filled with groundbreaking research, high profile panelists and even networking. For this blog, I’m going to focus on the networking, as this was the area that I was most skeptical of. How can you provide ample networking opportunities for clinicians, trainees and vendors when they’re all at home watching? Well, first, let me share the AHA’s plan to tackle this, then I’ll share some examples.
VIDEO: Networking Opportunities at AHA (Don Lloyd-Jones MD and Manesh Patel MD)
The AHA successfully delivered on their promise to fulfill the networking needs of its attendees in the following ways:
- AI-powered networking. The AHA brilliantly utilized burgeoning artificial intelligence technology to match like-minded individuals to each other as well as to programming that matched their interests. The AI then facilitated the organization of virtual meetings amongst interest-matched attendees. Wow!

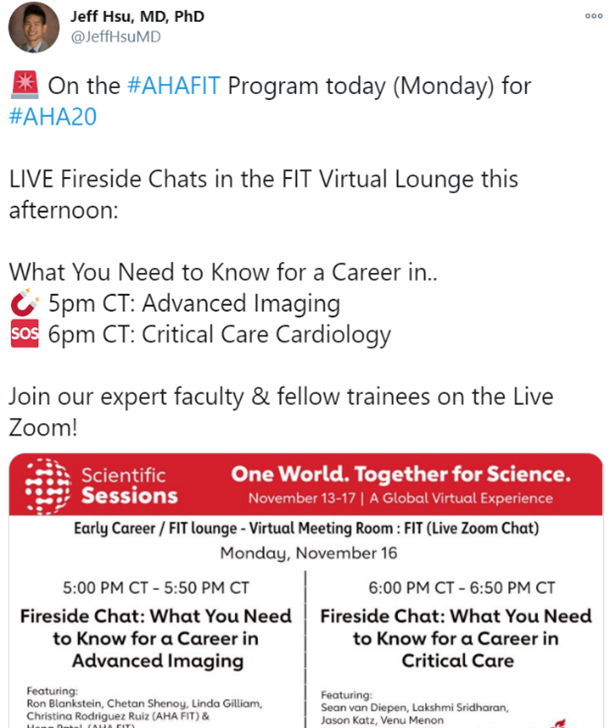
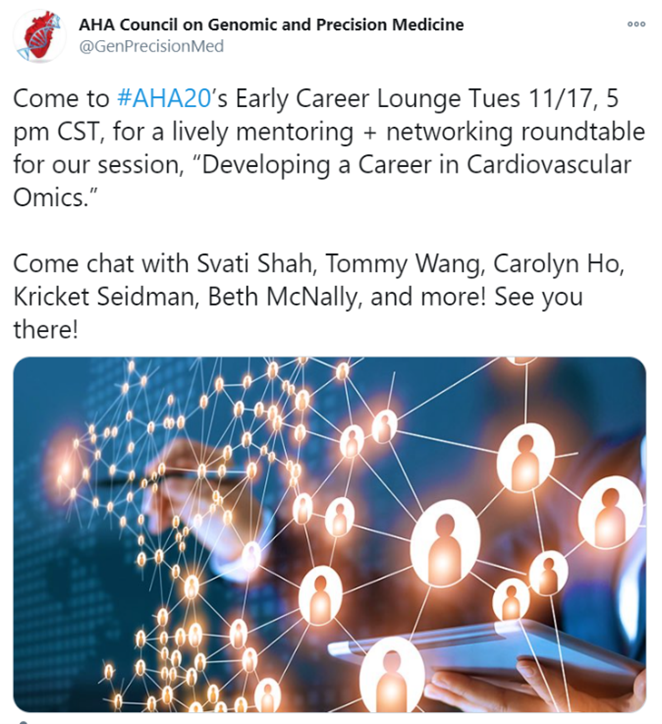
- Fireside chats and FIT Virtual Lounge. The AHA continued its focus on providing mentorship to early career cardiologists and trainees. The experience was as engaging, and some would argue more engaging, than the live sessions. The democratization of commentary afforded by virtual communication was evident, as even the most reserved participants were able to ask questions and exchange ideas with established leaders in the field.
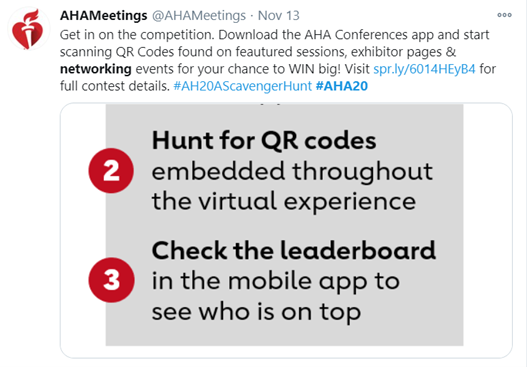
- Scavenger Hunt. Even the scavenger hunt was preserved! The AHA managed to provide a scavenger hunt experience via QR codes hidden throughout the conference programs for attendees to scan and WIN. This also further cultivated the relationship between the AHA and its industry partners.
- In line with its commitment to foster group wellness and health activities, the AHA organized morning yoga, exercise, and mental health sessions for attendees to virtually participate in together. This is a trend that has been popular since the start of the pandemic and hopefully will continue long after COVID-19 is gone.

In conclusion, my AHA 2020 experience has been rewarding in many ways. With quality education and networking opportunities, this year’s conference proved that the AHA is prepared to weather the challenges brought on by the COVID-19 pandemic. I look forward to future programming, and will certainly be an active participant.
“The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.”