2020 Was “Challenging and Creative” According to Dr. Harrington, How Would You Describe It?!
Everyone has different feelings about 2020 but I think it’s safe to say we have all taken the time to reflect on this past year and are filled with a new sense of hope for 2021. I sat down with Dr. Robert Harrington (past AHA President) to get his unique perspective on 2020 and what he looks forward to in 2021.

Dr. Robert Harrington, Immediate Past President, American Heart Association
Reflecting on 2020:
What went well in 2020 from the AHA? At the beginning of the pandemic, the AHA took a conscious effort to adapt as an organization. The AHA quickly pivoted its science and provided rapid response grants. Approximately 700 applications were submitted and the AHA fueled about 20 grants focusing on COVID research. The AHA also was seamlessly able to create a COVID registry based on our extensive experience with “get with the guidelines.” The organization continued to focus on being a voice for our patients with cardiovascular disease and wanting to bring quality evidence to clinicians – a few examples that come to mind include the debating of stopping ACE inhibitors and the effects of QT prolongation medications in patients with COVID.
What was the biggest change/disruption, how did you deal with it? As an academic clinical researcher, not being able to travel to meetings and conferences was very challenging. The meetings provide key networking that helps keep projects going but now we have less person-to-person contact. As AHA president, I wasn’t able to travel abroad to represent our organization and continue to build on our existing international relationships. Another change we also had to consider was how the pandemic and social distancing would affect the AHA 2020 sessions. Fortunately, our virtual platform was a success and we were continued to deliver pivotal science.
Looking forward to 2021:
How do you define success in 2021? Taking lessons on how to do things differently, for example, shifting to an online platform for fundraising and reviewing grants was successful. We were able to continue to do the work entrusted to us. We have embraced this shift in culture to help our organization grow and continue to be successful. We are also very exciting to see what will be discovered from the COVID registry.
What do you look forward to in the field of cardiology in 2021? The pandemic has fostered a lot of creativity. I think continued exploration in digital technology for patients with be key. Can we better control blood pressure, medication adherence, glucose control, etc via digital technology. This is an area of science and health care that is exponentially growing and it will be exciting to see what else we are able to develop.
Quick Tips for FIT:
How should FIT/Early career clinicians approach 2021? As we move back towards “normal” times, people need to take time off and decompress. We will find relief and gratitude we have gone through such a tremendous pandemic. It’s important to recognize burn-out and even more important for all of us to rejuvenate.
What do you think will cause the most stress and how can FIT/EC navigate it for a better future? My observation this past year (and during my time as an EC professional) it is the constant balance between professional vs personal life. During the pandemic, school closures and lack of elder care for example, have been a huge stressor on professionals. I hope we learned how to do things differently going forward to foster a better environment.
The memories of 2020 are still fresh in our minds but after speaking with Dr. Harrington, I too am more hopefully for a brighter, better, and as productive 2021. We have seen a tremendous growth in our community, compassion, and desire to help each other grow. So, good riddance to 2020 and cheers to 2021!
“The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.”
 Dr. Karen Griffin, who presented a seminar in April 2019 at the University of Tennessee Health Science Center (UTHSC) Department of Physiology, has carried the FAHA designation for several years, but now serves as Chair of the
Dr. Karen Griffin, who presented a seminar in April 2019 at the University of Tennessee Health Science Center (UTHSC) Department of Physiology, has carried the FAHA designation for several years, but now serves as Chair of the 

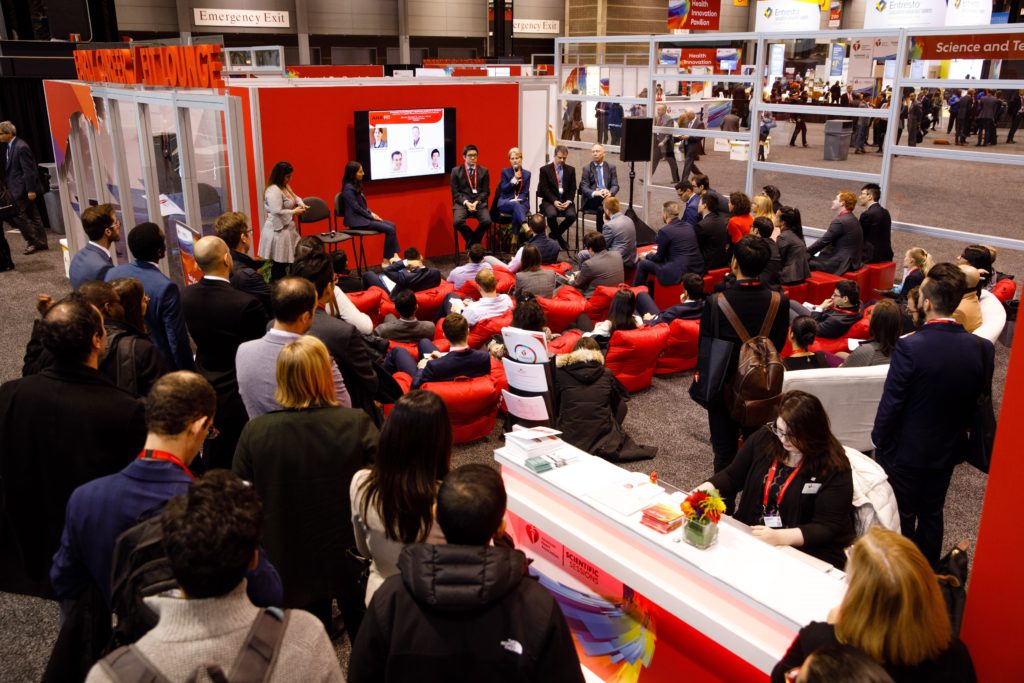

 At my first two AHA Scientific Sessions, I sat in the Main Event Hall, shoulder-to-shoulder with my co-fellows, eagerly awaiting the results of the Late Breaking Clinical Trials and guideline updates. I remember whispers cascading across the room after the presentation of NEAT-HFpEF in 2015 and the hundreds of cellphones in the air snapping pictures of the hypertension guideline release in 2017. This year as an AHA Early Career Blogger, I learned the results of the Late Breaking Clinical Trials with other news writers at embargoed media briefings. These intimate press conferences are routinely offered to health care journalists at major medical meetings and by top medical journals. Members of the media receive early access to manuscripts and data and discuss trial findings with investigators and outside experts with the understanding that nothing should be published until after trial results are publicly released. Generally, media pieces are published very soon after the embargo is lifted. At my first embargoed briefing, I heard one reporter’s question that has spurred me to imagine a new, more inclusive future for scientific meetings.
At my first two AHA Scientific Sessions, I sat in the Main Event Hall, shoulder-to-shoulder with my co-fellows, eagerly awaiting the results of the Late Breaking Clinical Trials and guideline updates. I remember whispers cascading across the room after the presentation of NEAT-HFpEF in 2015 and the hundreds of cellphones in the air snapping pictures of the hypertension guideline release in 2017. This year as an AHA Early Career Blogger, I learned the results of the Late Breaking Clinical Trials with other news writers at embargoed media briefings. These intimate press conferences are routinely offered to health care journalists at major medical meetings and by top medical journals. Members of the media receive early access to manuscripts and data and discuss trial findings with investigators and outside experts with the understanding that nothing should be published until after trial results are publicly released. Generally, media pieces are published very soon after the embargo is lifted. At my first embargoed briefing, I heard one reporter’s question that has spurred me to imagine a new, more inclusive future for scientific meetings. On Sunday of Sessions, I joined other health care reporters for the VITAL and REDUCE-IT presentations. In VITAL, 1 gram/day of omega-3 fatty acid supplementation (containing 460 mg of eicosapentaenoic acid [EPA] and 380 mg of docosahexaenoic acid [DHA]) was not effective for primary prevention of cardiovascular events in healthy middle-aged adults. In REDUCE-IT, icosapent ethyl (a purified EPA) at a dose of 2 grams twice daily reduced cardiovascular events among patients at risk for or with known cardiovascular disease and with high triglycerides already on statin therapy with good LDL-C control. After both trials were presented, one news writer probed the primary investigators’ thoughts on communicating these results to patients. The reporter wondered if the trials could be interpreted as sending mixed messages about the cardiovascular benefits of omega-3 fatty acids to the general public. Both trials’ primary investigators acknowledged this concern and systematically reviewed the differences in drug composition, patient populations, and study goals that, in their estimation, led to the outcomes. Multiple panelists implored the journalists to integrate these differences into their stories with hopes that consumers and potential patients would be able to understand the distinctions on their own.
On Sunday of Sessions, I joined other health care reporters for the VITAL and REDUCE-IT presentations. In VITAL, 1 gram/day of omega-3 fatty acid supplementation (containing 460 mg of eicosapentaenoic acid [EPA] and 380 mg of docosahexaenoic acid [DHA]) was not effective for primary prevention of cardiovascular events in healthy middle-aged adults. In REDUCE-IT, icosapent ethyl (a purified EPA) at a dose of 2 grams twice daily reduced cardiovascular events among patients at risk for or with known cardiovascular disease and with high triglycerides already on statin therapy with good LDL-C control. After both trials were presented, one news writer probed the primary investigators’ thoughts on communicating these results to patients. The reporter wondered if the trials could be interpreted as sending mixed messages about the cardiovascular benefits of omega-3 fatty acids to the general public. Both trials’ primary investigators acknowledged this concern and systematically reviewed the differences in drug composition, patient populations, and study goals that, in their estimation, led to the outcomes. Multiple panelists implored the journalists to integrate these differences into their stories with hopes that consumers and potential patients would be able to understand the distinctions on their own. After the briefing, I walked to the Main Event Hall to re-experience the Late Breaking Clinical Trials and thought about how we translate these breakthroughs, frequently announced at scientific meetings, to the public and our patients. Recent data suggest that the use of social media at cardiovascular conferences, a key approach to broadcasting late-breaking scientific developments, is rapidly growing. At these meetings, physicians comprise the largest group of Tweeters and compose nearly half of all tweets.1 Identifying the full scope of our social media audience, though, is more elusive. Ensuring veracity in scientific communication has become progressively challenging as the attitudes and tools to perpetuate misinformation have spread. We know that across multiple information domains, false news spreads faster, farther, and deeper than the truth.2 Just this week, Dictionary.com chose “misinformation” as the 2018 word of the year.3 Clinicians and scientists are now especially vulnerable to this insidious erosion of public trust.
After the briefing, I walked to the Main Event Hall to re-experience the Late Breaking Clinical Trials and thought about how we translate these breakthroughs, frequently announced at scientific meetings, to the public and our patients. Recent data suggest that the use of social media at cardiovascular conferences, a key approach to broadcasting late-breaking scientific developments, is rapidly growing. At these meetings, physicians comprise the largest group of Tweeters and compose nearly half of all tweets.1 Identifying the full scope of our social media audience, though, is more elusive. Ensuring veracity in scientific communication has become progressively challenging as the attitudes and tools to perpetuate misinformation have spread. We know that across multiple information domains, false news spreads faster, farther, and deeper than the truth.2 Just this week, Dictionary.com chose “misinformation” as the 2018 word of the year.3 Clinicians and scientists are now especially vulnerable to this insidious erosion of public trust. How do we combat the propagation of falsehood while encouraging this new democratization of science? I have thought about how the importance of trust was so admirably exemplified in a recent study of blood pressure reduction in black barbershops.4 What if we could leverage our meetings to spread science to where our patients are and with trusted people delivering the message? The AHA has recognized this opportunity and does have programs in place, like “Students at Sessions”, to share Scientific Sessions with non-medical communities.5 Can we imagine a future state of Scientific Sessions where internationally recognized clinicians and scientists deliver a talk at a barbershop or civic center in the host city, where community leaders are invited to participate in panels and plenaries, where large scale cardiovascular risk screenings happen just outside our conference center doors?
How do we combat the propagation of falsehood while encouraging this new democratization of science? I have thought about how the importance of trust was so admirably exemplified in a recent study of blood pressure reduction in black barbershops.4 What if we could leverage our meetings to spread science to where our patients are and with trusted people delivering the message? The AHA has recognized this opportunity and does have programs in place, like “Students at Sessions”, to share Scientific Sessions with non-medical communities.5 Can we imagine a future state of Scientific Sessions where internationally recognized clinicians and scientists deliver a talk at a barbershop or civic center in the host city, where community leaders are invited to participate in panels and plenaries, where large scale cardiovascular risk screenings happen just outside our conference center doors?