Heart Health and HIV: An Opportunity for Global Health Partnership
Slightly over five years ago, I immersed myself in a growing literature that documented the increase in heart disease in people living with HIV (PLHIV). While almost of all of these studies were in well-developed “high income” countries, the conclusion was always the same. The HIV medications worked, and those who had access to them were aging and developing conditions associated with aging including, prominently, cardiovascular disease (CVD). People living with HIV seemed to be developing these conditions more frequently than those who were not living with HIV, and no one was able to tease apart the myriad reasons why this was happening.
Global Burden of Atherosclerotic Cardiovascular Disease in People Living With HIV
DOI: (10.1161/CIRCULATIONAHA.117.033369
Others had the same realization and earlier this year. Anoop Shah, MD, from the University of Edinburgh, conducted the first meta-analysis examining the global burden of CVD in PLHIV. Pooling data from almost 800,000 PLHIV with 3.5 million person years of follow up, they found that the global burden of HIV-Associated CVD has tripled in the past 20 years, especially in low and middle-income nations.
Specifically, Dr. Shah and his team measured the population attributable fraction of CVD in PLHIV. This metric combines the risk associated with CVD with the prevalence of HIV- an approach that can quantify the actual impact of risk on a population. This is important because in low and middle-income countries where the HIV prevalence is high and resources are scarce, interventions to reduce the risk of CVD will likely have a bigger impact. Dr. Shah’s work revealed that those in sub-Saharan Africa experience a “double hit” of both HIV and CVD, with higher rates of traditional risk factors such as high blood pressure, and context-specific risk factors including air pollution.
To address these risk factors, Dr. Shah suggests that while there are studies leveraging cutting edge science to help us identify those living with or at risk for CVD (e.g. biomarkers), we need more research testing evidence-based strategies to improve cardiovascular outcomes in PLHIV in low and middle-income countries. This includes testing traditional pharmacological (e.g., antihypertensive and dyslipidemia) and non-pharmacological (e.g., diet, exercise and smoking cessation) strategies tailored to the setting and the population. Critically, this research must also account for the pivotal role health systems have in delivering these interventions.
This year the theme of World AIDS Day is “Building Partnerships through Leadership” and Dr. Shah captured this promise when discussing how to improve health systems to reduce CVD. “Based on my experience, in Sub-Saharan Africa HIV clinics are incredibly well run and effective, but they only do one thing- treat HIV; but what if we could partner with this HIV clinics across Africa [and other low and middle income settings] to start to provide better CVD prevention and treatment? By building on the existing systems, and expanding to other populations, we could deliver the change that is needed to improve cardiovascular health to PLHIV and beyond”.
Today is World AIDS Day and I am part of the first generation where AIDS has always existed. I was born a week after the MMRW report documented the first case of what would become known as AIDS. Since then we have made so much progress, and continue to make strides in preventing, treating, and eventually curing HIV. I look forward to the day when HIV will no longer be a part of anyone’s life. But until that happens, my work, and the work of many scientists, clinicians, advocates and allies will continue to build a better understanding of how to help all PLHIV enjoy the healthiest life possible, with less risk for cardiovascular diseases and stroke. By working with HIV organizations there are incredible opportunities for innovative and exciting partnerships to improve cardiovascular health in PLHIV, and millions of others around the globe. The American Heart Association can and should have an important role in this quest for longer, healthier lives.
Over the next year, I will explore what is known about the various causes of cardiovascular disease in this population in this series on Heart Health and HIV. I will work to incorporate high quality science with the perspectives of the both clinicians caring for PLHIV and the voices of the patients themselves. I look forward to engaging with all of you and, together, trying to solve these important issues.
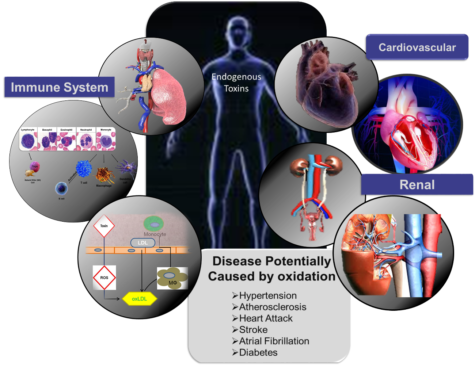
 Cardiovascular disease (CVD) remains the number one cause of mortality for both men and women in the United States1. Although CVD related mortality is decreasing with advanced diagnostic testing and therapies of CVD, the prevalence of this disease remains high including in the younger aged population younger than 55 years of age1. This suggests that as providers we have done a successful job at treating CVD however there remains a lot of work to be done with regards to preventing this disease.
Cardiovascular disease (CVD) remains the number one cause of mortality for both men and women in the United States1. Although CVD related mortality is decreasing with advanced diagnostic testing and therapies of CVD, the prevalence of this disease remains high including in the younger aged population younger than 55 years of age1. This suggests that as providers we have done a successful job at treating CVD however there remains a lot of work to be done with regards to preventing this disease.


 As serendipity will have it, I met a summer student while I was having lunch in the common break room (which I never do because who has time for lunch?). This student was studying
As serendipity will have it, I met a summer student while I was having lunch in the common break room (which I never do because who has time for lunch?). This student was studying