What do the guidelines say?
The 2017 AF guidelines give a Class IIa recommendation for performing a transesophageal echocardiogram (TEE) for patients with AF undergoing ablation who are in AF on presentation, even if they have been receiving therapeutic anticoagulation for 3 weeks or longer1. However, the more recent 2020 European College of Cardiology AF guidelines recommend therapeutic oral anticoagulation for at least 3 weeks before ablation (Class 1), or, use of TEE to exclude left atrial appendage thrombus before ablation2.
What is routine clinical practice?
In accordance with the guidelines, many centers, including our own, perform routine TEE before AF ablation, however, my recent Twitter poll suggests that there is wide variation in clinical practice3 (Figure 1). The benefit of performing this TEE is the ability to rule out left atrial and left atrial appendage (LAA) thrombus. However, the routine use of TEE not only adds to the overall risk of the ablation but also increases the cost of care.
Why this practice should be questioned?
There have been multiple changes in recent years that have questioned the role of routine TEE before AF ablation. These include:
1) The advent of direct oral anticoagulants (DOACs) that have better efficacy and safety than warfarin.
2) Increasing preference and guideline recommendations endorsing the practice of uninterrupted DOACs before ablation that has shown to be associated with very low rates of peri-procedural thromboembolic complications.
3) Availability and use of intracardiac echocardiography (ICE) that can be used to rule out LAA thrombus.
What does recent data suggest? (Figure 2)
The September 2020 issue of Circulation Arrhythmia and Electrophysiology had a very interesting study by Diab et al asking this important clinical question4. In their analysis of 900 patients presenting with AF or atrial flutter for ablation who did not undergo any pre-procedural or intraprocedural imaging for the purpose of ruling out LAA thrombus and were taking uninterrupted DOACs for > 3 weeks, they found that only 4 (0.3%) patients developed thromboembolic complications with 2 ischemic strokes, 1 transient ischemic attack (TIA) and 1 splenic infarct. The authors concluded that in patients taking uninterrupted DOACS and undergoing AF/atrial flutter ablation, omitting the pre-procedural TEE and ICE from the right ventricular outflow tract was feasible and associated with a low risk of thromboembolic complications.
Similar results were observed in the much large multicenter prospective registry data of over 6000 patients by Patel et al5 where only 1 TIA was observed in the setting of a missed dose of Rivaroxaban before ablation. However, in this study ICE ruled out LAA thrombi in all patients in contrast to the study by Diab et al where ICE was not used.
Take Home Message
Recent data from two large observational studies suggest that in patients with AF who are undergoing ablation and taking uninterrupted DOAC for at least > 3 weeks before ablation, performing a pre-procedural TEE is not necessary. Given the very low event rates of thromboembolic complications during ablation, the feasibility of a large randomized trial addressing this specific question seems uncertain as it will require a very large sample size.
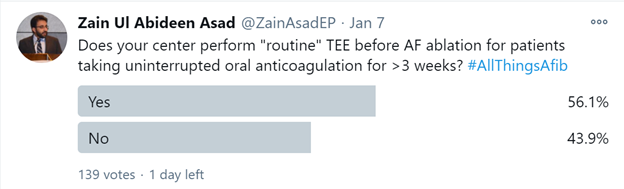
Figure 1: Twitter poll showing the equipoise on performing routine transesophageal echocardiogram (TEE) in patients undergoing catheter ablation of atrial fibrillation.
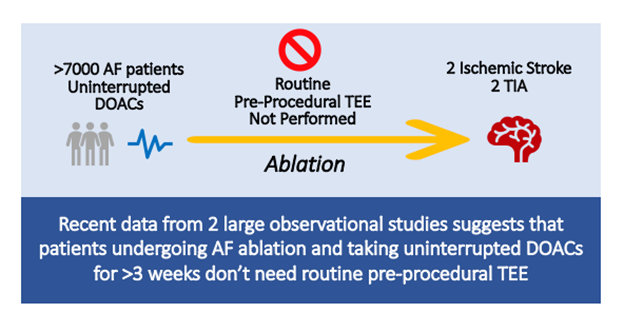
Figure 2: Summary of data from 2 recent large observational studies suggesting that omitting routine transesophageal echocardiogram (TEE) is safe
REFERENCES
- Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace. 2018;20(1):e1-e160. doi:10.1093/europace/eux274
- Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. Published online August 29, 2020. doi:10.1093/eurheartj/ehaa612
- Asad Z. Does your center perform “routine” TEE before AF ablation for patients taking uninterrupted oral anticoagulation for >3 weeks? https://twitter.com/ZainAsadEP/status/1347349701067206656?s=20
- Diab Mohamed, Wazni Oussama M., Saliba Walid I., et al. Ablation of Atrial Fibrillation Without Left Atrial Appendage Imaging in Patients Treated With Direct Oral Anticoagulants. Circulation: Arrhythmia and Electrophysiology. 2020;13(9):e008301. doi:10.1161/CIRCEP.119.008301
- Patel K, Natale A, Yang R, et al. Is transesophageal echocardiography necessary in patients undergoing ablation of atrial fibrillation on an uninterrupted direct oral anticoagulant regimen? Results from a prospective multicenter registry. Heart Rhythm. 2020;17(12):2093-2099. doi:10.1016/j.hrthm.2020.07.017
“The views, opinions and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your personal health matters. If you think you are having a heart attack, stroke or another emergency, please call 911 immediately.”