Over the history of echocardiography, there have been a multitude of research studies on the feasibility, reproducibility and the prognostic values of different echocardiographic parameters in different disease groups. Fifty years later, no single echocardiographic parameter is unique for assessment of the cardiac structure and function. Even the most widely used measurement for left ventricle ejection fraction (LVEF) has important limitations, including low sensitivity for incident heart failure (HF), specifically HF with preserved ejection fraction (HFpEF). With the advent of speckle tracking echocardiography (STE), early detection of cardiac dysfunction before signs or symptoms of HF develop (stage A or B HF) has become a target of many researchers in the last 15 years. Although, there has been some success, there is still a long way to go. In this blog, I want to discuss the differences, advantages and the limitations of mitral annular plane systolic excursion (MAPSE) vs. global longitudinal strain (GLS).
MAPSE measures LV longitudinal shortening and it has been around for over 50 years. Reduction in MAPSE was described as a marker of LV dysfunction (Figure 1). Nowadays, newer and more refined echocardiographic technologies, such as strain, are used more widely for assessment of LV function and deformation. STE imaging has been around for quite a while and we celebrated it’s first decade just 4 years ago, whereas the technique described in 2004 (Leitman M-JASE) and clinical applications appeared around 2005 (Notomi Y- JACC). Since then, the interest has risen dramatically and so far, we have around 6,000 publications on this topic. GLS is the most studied among strain parameters and its prognostic value has been demonstrated in several clinical scenarios.
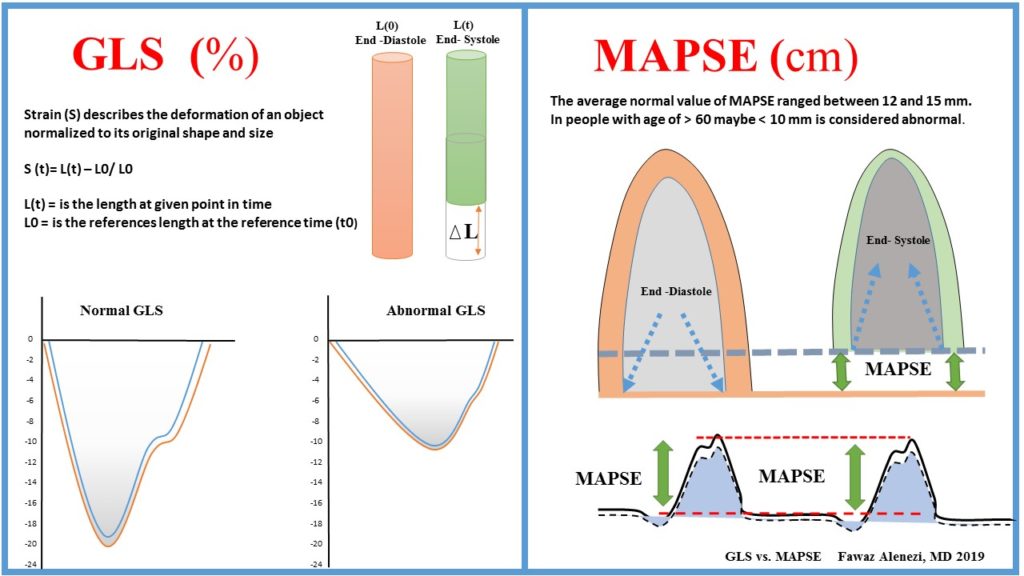
Figure 1: GLS vs. MAPSE – Fawaz Alenezi -2019.
| MAPSE (cm) | GLS (%) | |
|
Technique |
|
|
| Advantages |
|
|
| Disadvantages |
|
|
Table 1: Advantages and limitations of GLS vs. MAPSE- Fawaz Alenezi – 2019
What is thought to be the main advantage of STE over MAPSE is the ability of global and regional function assessment. However, with regard to regional (segmental) function, I think this is more challenging and there is still progress to be made. The challenges exist because we have only one segment to work with and less data to average. Tracking quality becomes more important, regional artifacts matters more, definition of sample position more relevant, and more importantly, we cannot simply measure peak values anymore. For regional analysis, the strain curve shape (not peak values, because peak values can be the same) become critical. Regional strain measurements have much higher variability among vendors when compared with GLS. Recently, the HUNT study (Stoylen A et al. 2018 –Wiley echocardiography journal) showed that MAPSE and GLS measured both as MAPSEn (n= normalized for end diastolic length) and GLS have similar biological variability in adults without improvement by normalizing for length for both.
In summary, I think both GLS and MAPSE are measuring the same cardiac function. GLS is robust, reproducible and has been shown to add unique data that can guide diagnosis and management. However, it is vendor, image quality and hemodynamics dependent that need more standardization and experience. On the other hand, MAPSE is simple, easy, available in every echo machine and, more importantly, feasible even in a poor image quality. But it is not measuring the global function. Further studies are needed to standardize vendors, recognize specific strain patterns, determine if there is loading conditions difference and head-to-head comparison between both methods.