My First Year As An Attending – What I have learned
After many years of training, it finally happened, I was going to be an attending. The goal we all strive for – to take the training wheels off, practice what we learned, and provide the best care possible for our patients. I spent months leading up to my first week on service incredibly nervous and found myself reviewing guidelines, trials, and any other resource to help me succeed – safe to say, I was psyching myself into a frenzy.
Like many of us, the fear of failure is an incredibly motivating factor but perhaps not the healthiest mindset. I’d like to share my journey as a first-year attending and what I learned in hopes of helping others who are finally taking off the training wheels.
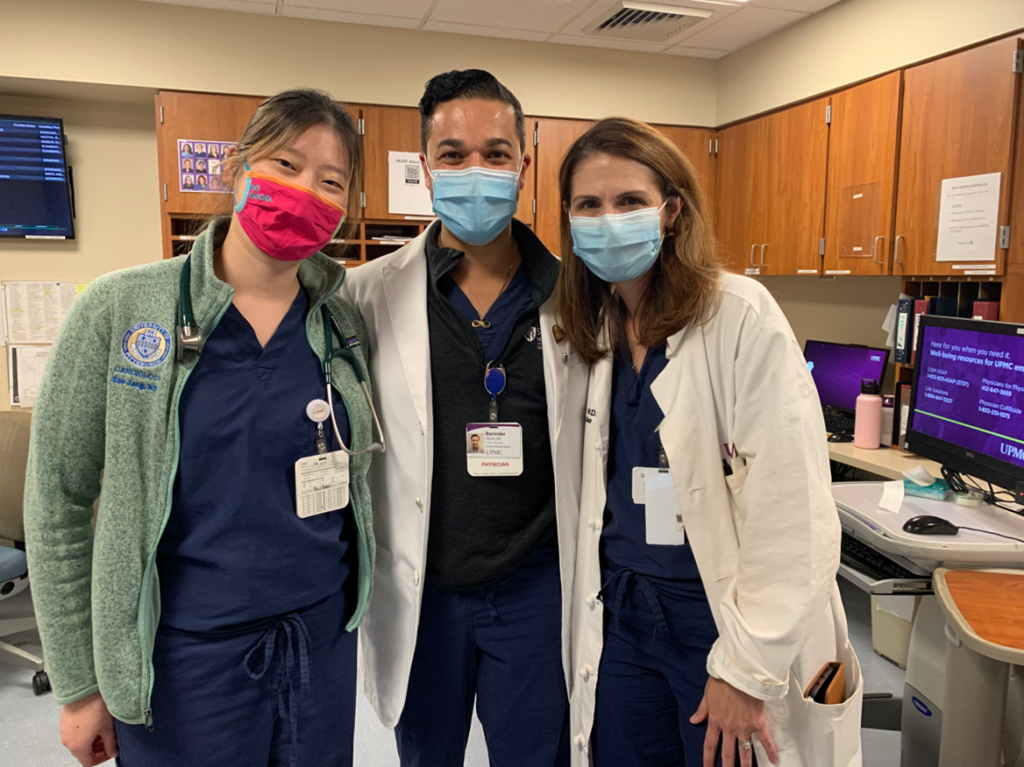
Day 1 as attending, celebrating great news our patient was undergoing heart transplant.
1. Your department wants you to be successful. It may feel like you are alone as an attending, but your department invested a lot of time and resources for you to join. They want you to succeed and encourage open lines of communication. The senior members in both my departments (cardiology and critical care) expected me to call them when I was struggling with a challenging case, needed clarity on how to navigate the new system I was working in, and to touch base on how I was doing. I have called my colleagues on the weekends and at odd hours to ensure I was providing the best care for my patients – and the best part, they did not once make me feel inferior or as if I was doing a bad job.
2. Push your socializing boundaries. When I started working for UPMC, I only knew the handful of people who interviewed me. Many of my colleagues knew who I was through the continued updates from our division leadership regarding new hires but to me, everyone was a stranger. The best way I can describe it is as a year of continued blind-dating. I would meet faculty members, make small talk, and then move on.
I, therefore, made it a mission to get to know as many people as possible. I would introduce myself to all of the nursing staff in the mornings when I would see patients. This gave me a chance to get to know my CICU/CTICU team and get updates on the patients. When I would meet other attendings (in cardiology and critical care), I would introduce myself and get their phone number. I took the same approach for attendings who were consulting on my patients so I could continue to develop relationships across the health care system.
I’m fortunately a very social person, so this was not a terribly big challenge but if you are a bit shyer, this may very well feel uncomfortable and awkward. Keep in mind, that your colleagues want to get to know you (as you are the newest hire) but you have to get to know an entire division’s worth of faculty. Plus, if you throw in the trainees it becomes an even bigger task.

Supporting Go Red For Women with the entire CTICU Team
3. Don’t be afraid to ask for help. In order to be successful, don’t be afraid to ask for help, whether that is related to patient or personal care. Being a new attending has numerous challenges but asking for help isn’t one of them. I remember a difficult case being evaluated amongst our cardiogenic shock team to discuss the possibility of placing a patient on ECMO. I wasn’t sure the best course of action as I was the attending in the CTICU that week and my input would be heavily weighed. I immediately reached out to our CTICU Medical Director to hop on the call. He was able to give his insight on the case, which helped us determine a better clinical course. I was able to debrief with him afterward and learned for the next time I would encounter a similar situation.
4. Don’t forget your past mentors. Many of us will start working as hospitals we have never stepped foot in. Our past relationships are of incredible value. I still text and call my mentors for advice. They are a great objective 3rd party to speak to.
5. Enjoy the process. Being an attending is hard but remember the years of training you have completed getting to this point. We became physicians to accomplish a variety of goals (research, clinical care, etc) and we are well trained for it.
Although the training wheels may have come off and I am no longer considered a trainee, I make sure I am diligent in growing and learning at every opportunity. I’ve learned so much in my first year as an attending and can’t wait to see what else is in store.
“The views, opinions, and positions expressed within this blog are those of the author(s) alone and do not represent those of the American Heart Association. The accuracy, completeness, and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions, or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them. The Early Career Voice blog is not intended to provide medical advice or treatment. Only your healthcare provider can provide that. The American Heart Association recommends that you consult your healthcare provider regarding your health matters. If you think you are having a heart attack, stroke, or another emergency, please call 911 immediately.”




 I also spoke to several of my co-fellows which turned into all of us sharing where we have interviewed or places we think the other may find as a good fit. Don’t be afraid to reach out if you’re in this position – you have nothing to lose but a lot to gain! Reaching out to mentors is also important as they may have leads on jobs you may not have considered before.
I also spoke to several of my co-fellows which turned into all of us sharing where we have interviewed or places we think the other may find as a good fit. Don’t be afraid to reach out if you’re in this position – you have nothing to lose but a lot to gain! Reaching out to mentors is also important as they may have leads on jobs you may not have considered before. James Derham (or perhaps it was Durham) is believed to be the first Black person to officially practice medicine in the U.S and without a medical degree. It is believed he learned by way of apprenticeships which was a major form of passing skills to those who didn’t (or couldn’t) attend university. He was born a slave and worked for many doctors. He was able to buy his freedom and continue to practice, but by the early 1800s, James disappears from history. Some say he was murdered and others believe he left Philadelphia to practice medicine elsewhere.
James Derham (or perhaps it was Durham) is believed to be the first Black person to officially practice medicine in the U.S and without a medical degree. It is believed he learned by way of apprenticeships which was a major form of passing skills to those who didn’t (or couldn’t) attend university. He was born a slave and worked for many doctors. He was able to buy his freedom and continue to practice, but by the early 1800s, James disappears from history. Some say he was murdered and others believe he left Philadelphia to practice medicine elsewhere. Vivien Theodore Thomas was born in New Iberia, Louisiana and attending high school in Nashville in the 1920s. Vivien always wanted to be a doctor but due to the Great Depression he was forced to work instead. He eventually, became an assistant to surgeon Alfred Blalcok – most noted for his work in shock and Tetralogy of Fallot. Their hard work (along with Dr. Helen Taussig) created the Blalock-Thomas-Taussig Shunt, an operation that ushered in the modern era of cardiac surgery. In 1976, Vivien was awarded an honorary doctorate and named an instructor for surgery at Johns Hopkins School of Medicine. A great movie I saw about Vivien was Something the Lord Made and highly recommend it.
Vivien Theodore Thomas was born in New Iberia, Louisiana and attending high school in Nashville in the 1920s. Vivien always wanted to be a doctor but due to the Great Depression he was forced to work instead. He eventually, became an assistant to surgeon Alfred Blalcok – most noted for his work in shock and Tetralogy of Fallot. Their hard work (along with Dr. Helen Taussig) created the Blalock-Thomas-Taussig Shunt, an operation that ushered in the modern era of cardiac surgery. In 1976, Vivien was awarded an honorary doctorate and named an instructor for surgery at Johns Hopkins School of Medicine. A great movie I saw about Vivien was Something the Lord Made and highly recommend it. Rebecca Lee Crumpler was an American nurse, physician, and later turned author. She is believed to be the first African American woman to become a doctor of medicine in the U.S, studying at New England Female Medical College. In 1883, she wrote Book of Medical Discourses dedicated to maternal and pediatric medical care. It was the first publications written by an African American about medicine. After the Civil War, she continued to treat women and children in Virgina. She also worked for the Freedmen’s Bureau to provide medical care for freed slaves.
Rebecca Lee Crumpler was an American nurse, physician, and later turned author. She is believed to be the first African American woman to become a doctor of medicine in the U.S, studying at New England Female Medical College. In 1883, she wrote Book of Medical Discourses dedicated to maternal and pediatric medical care. It was the first publications written by an African American about medicine. After the Civil War, she continued to treat women and children in Virgina. She also worked for the Freedmen’s Bureau to provide medical care for freed slaves. Edith Mae Irby was inspired to become a physician after unfortunately seeing her sister pass from typhoid fever. At a young age, she saw health care disparities first hand and believed her sister passed prematurely due to lack of care because her family was poor. This sparked a fire for Edith to become a physician that found her reward in service not wealth. Edith was the first African-American student admitted to the University of Arkansas Medical School in 1948 and believed to be the first black student enrolled in any all-white medical school in the South. This comes 6 years before the Supreme Court’s decision on Brown v Board of Education.
Edith Mae Irby was inspired to become a physician after unfortunately seeing her sister pass from typhoid fever. At a young age, she saw health care disparities first hand and believed her sister passed prematurely due to lack of care because her family was poor. This sparked a fire for Edith to become a physician that found her reward in service not wealth. Edith was the first African-American student admitted to the University of Arkansas Medical School in 1948 and believed to be the first black student enrolled in any all-white medical school in the South. This comes 6 years before the Supreme Court’s decision on Brown v Board of Education.